
Pancreatic Surgery — MCQs

On this page
What is the most common type of pancreatic tumor?
Which of the following is NOT true for annular pancreas?
A 66-year-old man presents with obstructive jaundice and is found on ERCP to have periampullary carcinoma. He is otherwise in excellent physical condition with no evidence of metastasis. What is the most appropriate treatment?
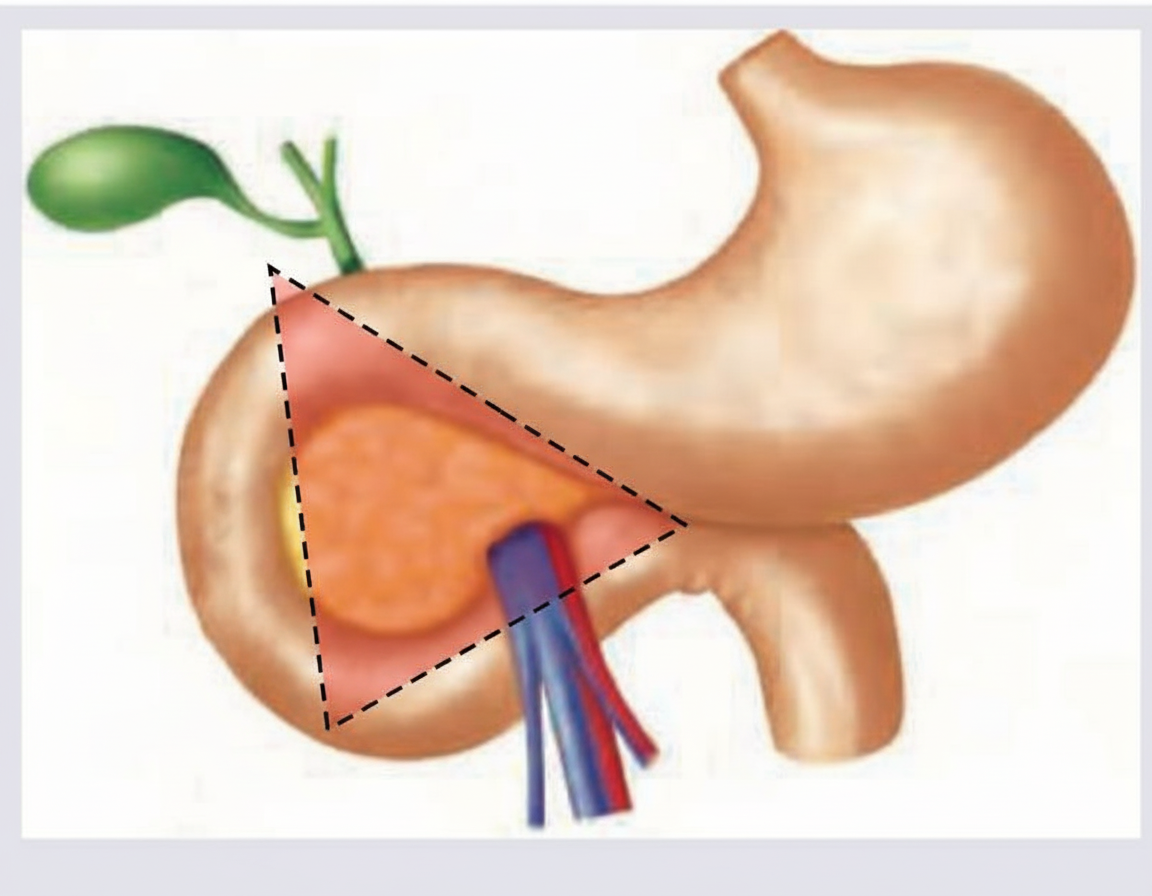
Which tumor is commonly seen in the area marked below?
A 40-year-old alcoholic presents with severe epigastric pain and hemodynamic collapse persisting for more than 48 hours despite adequate fluid resuscitation. CT abdomen was performed after fluid resuscitation which shows: (Recent NEET Pattern 2016-17)

A 30-year-old alcoholic presented with features of acute abdomen. Examination finding is shown below. What is the diagnosis?

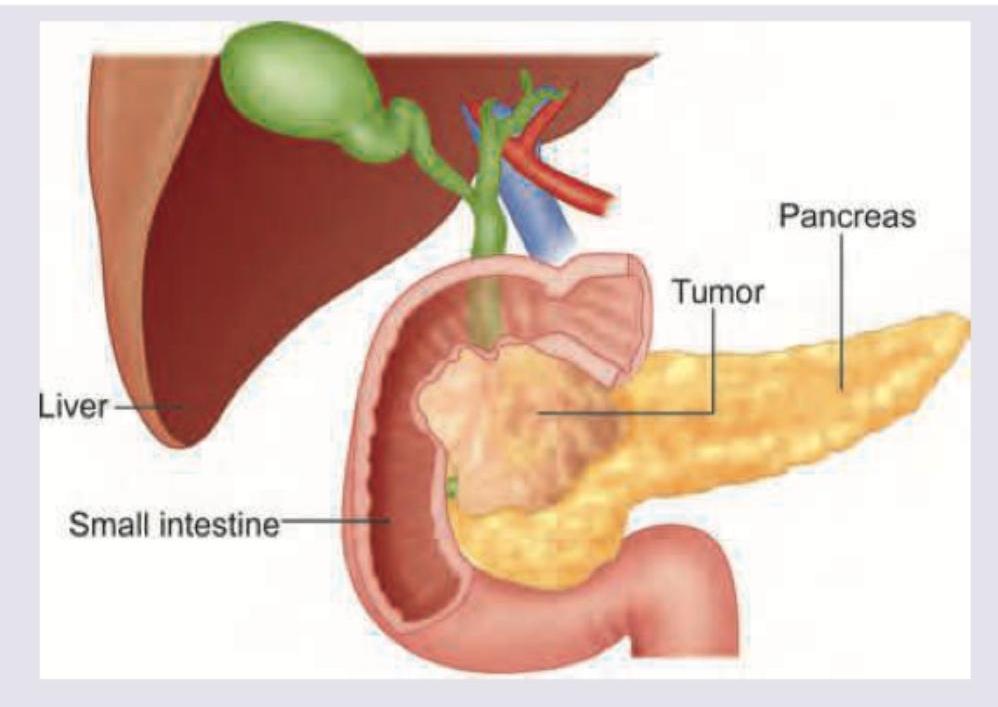
A patient with obstructive jaundice has the following imaging findings suggestive of pancreatic cancer. Which is the most appropriate method for obtaining tissue diagnosis?
Which of the following are local complications of acute pancreatitis? 1. Pseudocyst 2. Pleural effusion 3. Ileus 4. Acute fluid collection Select the correct answer using the code given below.
Which of the following is included in Ranson scoring system to predict the severity of acute pancreatitis at the time of admission? A. WBC count > 15 x 10^3/L B. Blood glucose > 200 mg/dL C. LDH > 350 units/L D. AST > 250 units/L
Which of the following scoring systems are PRIMARILY designed for assessing the severity of acute pancreatitis?
Practice by Chapter
Pancreatic Anatomy and Physiology
Practice Questions
Acute Pancreatitis
Practice Questions
Chronic Pancreatitis
Practice Questions
Pancreatic Pseudocysts
Practice Questions
Pancreatic Adenocarcinoma
Practice Questions
Cystic Neoplasms of Pancreas
Practice Questions
Neuroendocrine Tumors of Pancreas
Practice Questions
Pancreatic Trauma
Practice Questions
Pancreatectomy Techniques
Practice Questions
Whipple Procedure
Practice Questions
Pancreatic Anastomosis
Practice Questions
Complications of Pancreatic Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app