
Pancreatic Surgery — MCQs

On this page
Which of the following is NOT a risk factor for post-ERCP pancreatitis?
What is the gold standard investigation for chronic pancreatitis?
All are true about Zollinger-Ellison syndrome except?
All of the following can be used to predict severe acute pancreatitis except?
Which of the following is NOT an operation for chronic pancreatitis?
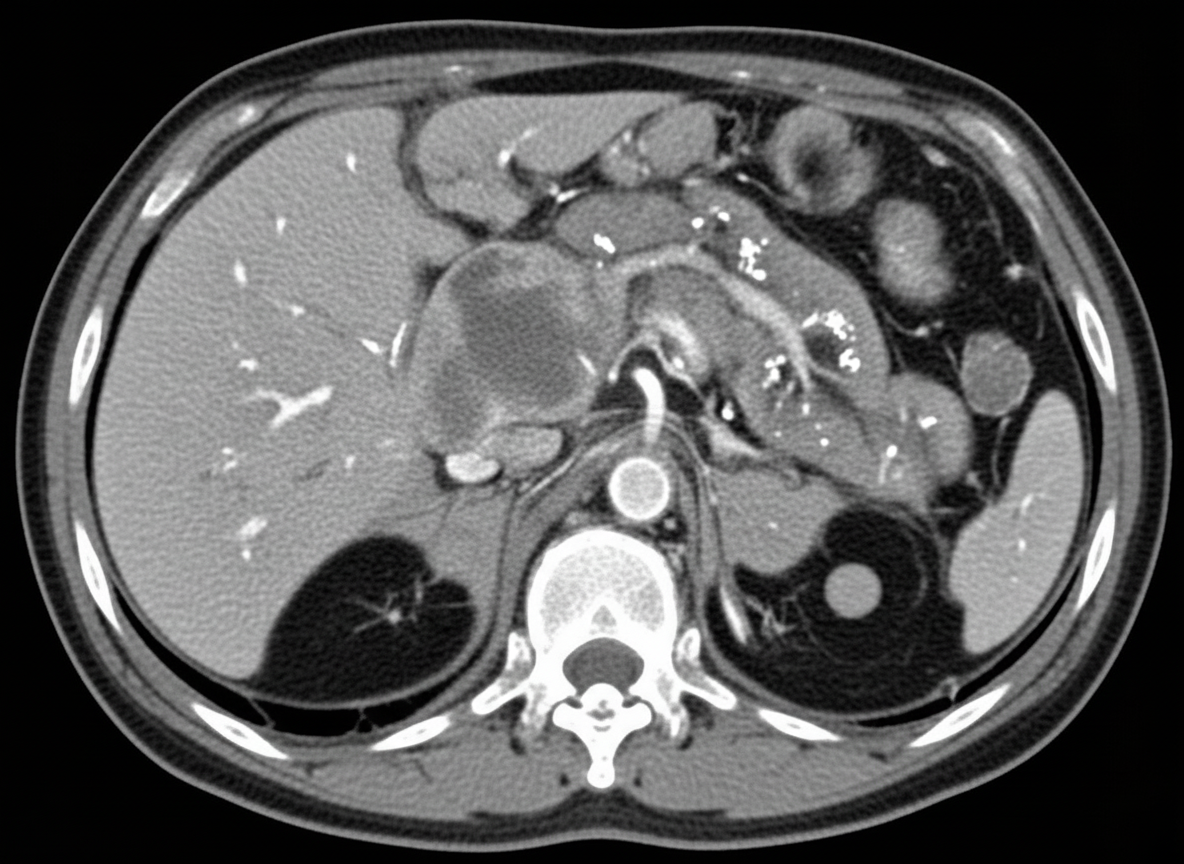
A 60-year-old woman with a history of chronic pancreatitis presents with worsening epigastric pain radiating to the back, accompanied by nausea and vomiting. She has experienced a 10 kg weight loss over the past 4 months. There is no evidence of jaundice, and liver function tests and serum amylase/lipase levels are within normal limits. A CT scan of the abdomen reveals a pancreatic head mass with greater than 180-degree superior mesenteric artery encasement and multiple hepatic metastases. Histologic confirmation of malignancy has been obtained. What is the most appropriate overall treatment strategy for this patient?
What is the most common site of ectopic pancreas?
Which of the following laboratory findings or scoring systems indicates severe pancreatitis?
What is the primary management of a pancreatic abscess?
What is the treatment of choice for cancer of the head of the pancreas?
Practice by Chapter
Pancreatic Anatomy and Physiology
Practice Questions
Acute Pancreatitis
Practice Questions
Chronic Pancreatitis
Practice Questions
Pancreatic Pseudocysts
Practice Questions
Pancreatic Adenocarcinoma
Practice Questions
Cystic Neoplasms of Pancreas
Practice Questions
Neuroendocrine Tumors of Pancreas
Practice Questions
Pancreatic Trauma
Practice Questions
Pancreatectomy Techniques
Practice Questions
Whipple Procedure
Practice Questions
Pancreatic Anastomosis
Practice Questions
Complications of Pancreatic Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app