
Pancreatic Surgery — MCQs

On this page
A patient with a known history of gallstones presents with severe abdominal pain and elevated serum lipase levels, along with periumbilical ecchymosis. Which of the following values helps to predict the severity of the condition, except?
Whipple's triad in insulinoma includes all of the following EXCEPT:
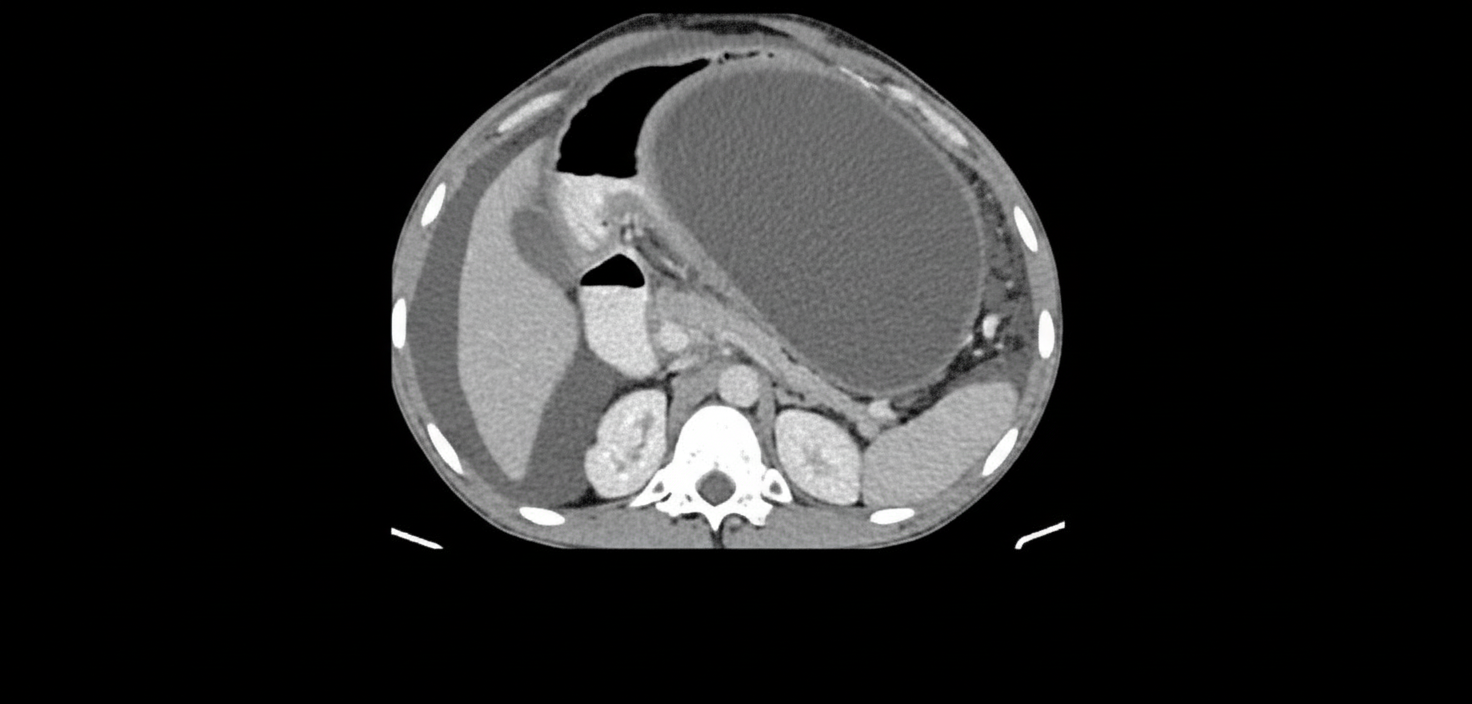
A 30-year-old patient presents with severe upper abdominal pain and elevated serum lipase. This is day 2 of the illness. A CECT scan was performed and is shown, demonstrating an early acute pancreatic fluid collection without an encapsulated wall, no necrotic contents, no signs of infection, no obstruction, and no persistent symptoms beyond the acute presentation. What is the next line of management?
The "chain of lakes appearance" on ERCP is typically seen in which of the following conditions?
All of the following are true about pancreatic cancer, EXCEPT:
Which of the following is FALSE about annular pancreas?
Which of the following criteria is NOT included in Ranson's criteria for predicting the severity of pancreatitis?
Whipple's operation is done for the treatment of which condition?
Localization in insulinoma is best with:
A 50-year-old lady presents with a 2-year history of recurrent abdominal pain radiating to her back. The pain is severe and refractory to simple analgesics. Ultrasound abdomen and contrast-enhanced CT scan confirmed the diagnosis and showed a dilated pancreatic duct. Which of the following is the likely recommended surgical procedure of choice?
Practice by Chapter
Pancreatic Anatomy and Physiology
Practice Questions
Acute Pancreatitis
Practice Questions
Chronic Pancreatitis
Practice Questions
Pancreatic Pseudocysts
Practice Questions
Pancreatic Adenocarcinoma
Practice Questions
Cystic Neoplasms of Pancreas
Practice Questions
Neuroendocrine Tumors of Pancreas
Practice Questions
Pancreatic Trauma
Practice Questions
Pancreatectomy Techniques
Practice Questions
Whipple Procedure
Practice Questions
Pancreatic Anastomosis
Practice Questions
Complications of Pancreatic Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app