
Pancreatic Surgery — MCQs

On this page
Match each of the following clinical conditions with its most appropriate diagnostic investigation: Clinical Condition Investigation A. Pancreatic pseudocyst 1. FNAC B. Thyroid nodule 2. MRCP C. Prostate cancer 3. PET scan D. Obstructive jaundice 4. CT scan Which of the following is the correct match?
Pancreatic pseudocyst most commonly occurs after which condition?
What is the commonest cyst to arise in the pancreas after an attack of acute pancreatitis or pancreatic trauma?
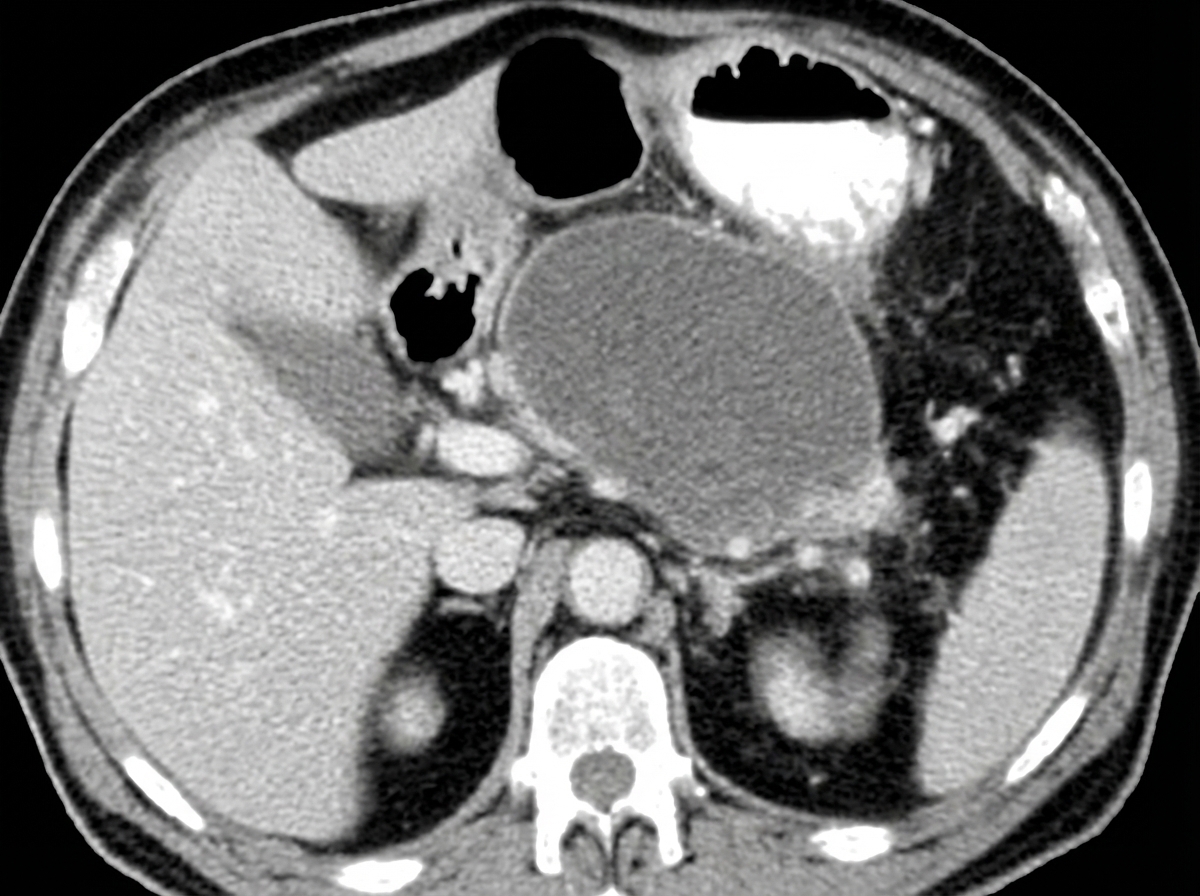
A chronic alcoholic presented with repeated episodes of non-bilious vomiting after meals. Based on CECT findings, what is the diagnosis?
Which branch of the portal vein is involved in chronic pancreatitis?
Which of the following statements is NOT true regarding a pseudocyst of the pancreas?
Which statement is NOT true regarding insulinoma?
All of the following are known complications of pancreatitis except?
What is the investigation of choice to detect gastrinoma less than 5 mm in size?
Which of the following best assesses the severity of pancreatitis?
Practice by Chapter
Pancreatic Anatomy and Physiology
Practice Questions
Acute Pancreatitis
Practice Questions
Chronic Pancreatitis
Practice Questions
Pancreatic Pseudocysts
Practice Questions
Pancreatic Adenocarcinoma
Practice Questions
Cystic Neoplasms of Pancreas
Practice Questions
Neuroendocrine Tumors of Pancreas
Practice Questions
Pancreatic Trauma
Practice Questions
Pancreatectomy Techniques
Practice Questions
Whipple Procedure
Practice Questions
Pancreatic Anastomosis
Practice Questions
Complications of Pancreatic Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app