
Laparoscopic Access Techniques — MCQs

Which of the following surgical incisions is associated with the highest risk of postoperative pulmonary complications ?
Endotracheal tube in the esophagus is best assessed by:
What is the most common site of ligation by laparoscopic ring in female sterilization?
Which of the following is a primary aim of damage control laparotomy?
To minimize ureteric damage, the following preoperative and operative precautions may be taken except:
The best investigation for air in the peritoneal cavity is:
A 25-year-old male presents with inguinal swelling. He had surgery for acute abdomen 2 years ago but could not tell the reason behind it. Trauma to which structure during the surgery conducted 2 years ago would have resulted in this inguinal swelling?
Most commonly ruptured organ in blunt trauma to abdomen is:
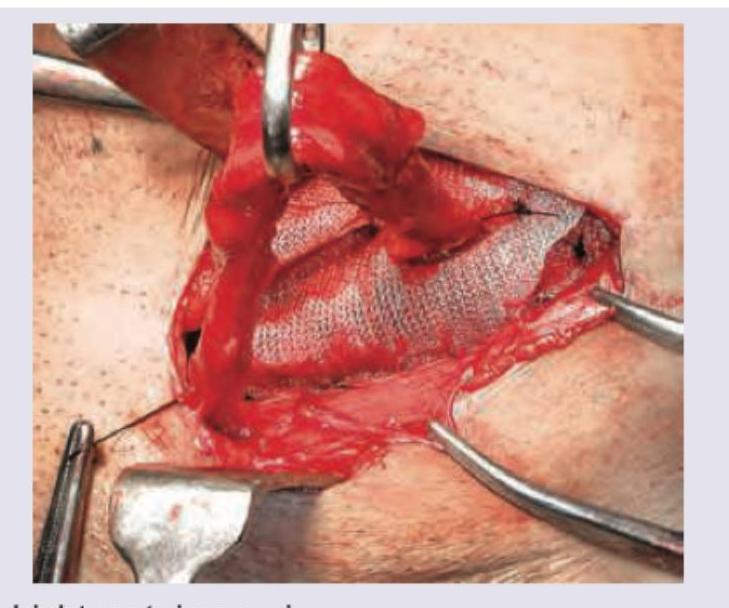
Which hernia repair procedure is shown in the image? (Recent NEET Pattern 2016-17)
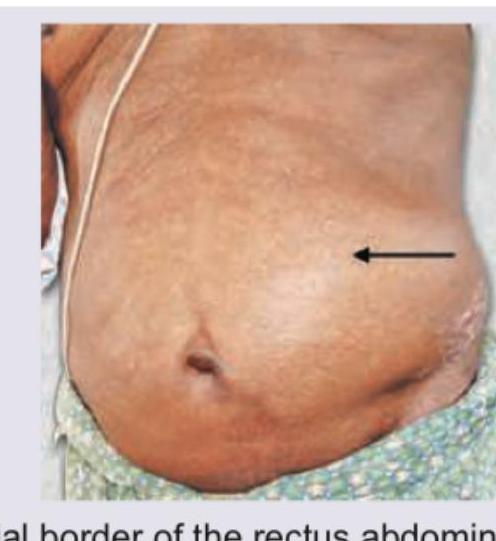
Hernia that is depicted in the image usually occurs at:
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app