
Hepatobiliary Surgery — MCQs

On this page
The following conditions are associated with high incidence of pigment gallstones except:
In gallstone ileus, obstruction most frequently occurs at:
A 45-year-old woman undergoes laparoscopic cholecystectomy. On postoperative day 3, she develops right upper quadrant pain, fever, and jaundice. Her bilirubin rises from 1.2 to 8.5 mg/dL. ERCP shows extravasation of contrast from the common bile duct. What is the most likely cause of this complication?
A 65-year-old man with cirrhosis (Child-Pugh B) and hepatocellular carcinoma presents with a 4 cm tumor. He has portal hypertension with esophageal varices and ascites. His MELD score is 18. Evaluate the optimal treatment strategy considering tumor stage, liver function, and available therapies.
A 72-year-old man with severe coronary artery disease, ejection fraction 25%, and recent MI 6 weeks ago presents with acute cholangitis (Charcot's triad). Blood cultures grow E. coli, and ERCP shows choledocholithiasis with biliary obstruction. His surgical risk is prohibitive. Evaluate the best management strategy that balances infection control, biliary drainage, and cardiac risk.
A patient is found to have an asymptomatic common bile duct (CBD) stone two years after cholecystectomy on routine imaging. What is the most appropriate initial management?
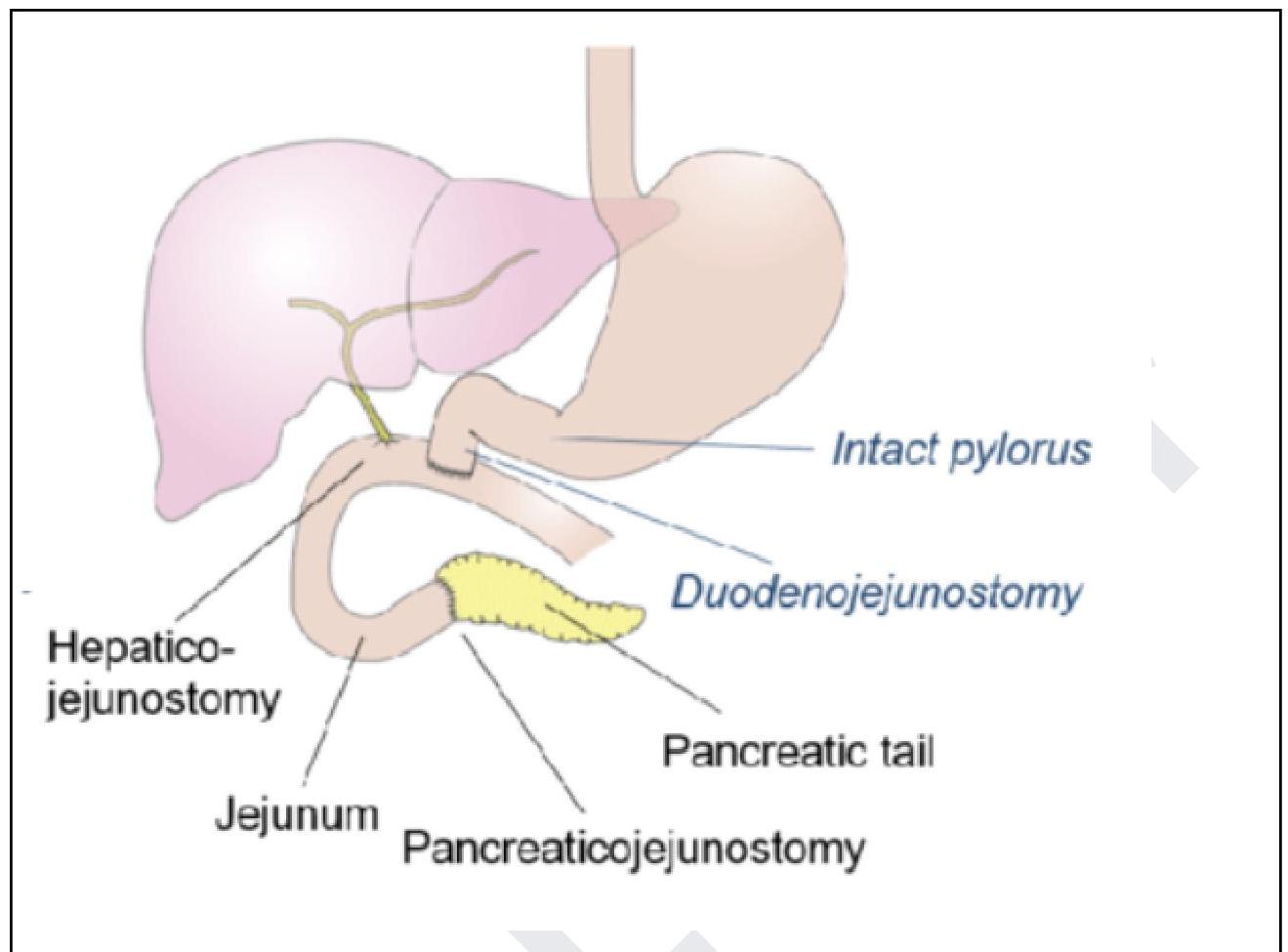
A 58-year-old man presents with progressive obstructive jaundice and weight loss. MRCP reveals a stricture in the distal common bile duct with no pancreatic duct dilation or calcifications. The following procedure is performed for the management of?
All the following are true about acute cholecystitis, except
A 34-year-old patient presents with severe pain in the right upper quadrant that radiates to the right shoulder. During laparoscopic cholecystectomy, which of the following anatomical spaces must be carefully identified to prevent bile duct injury?
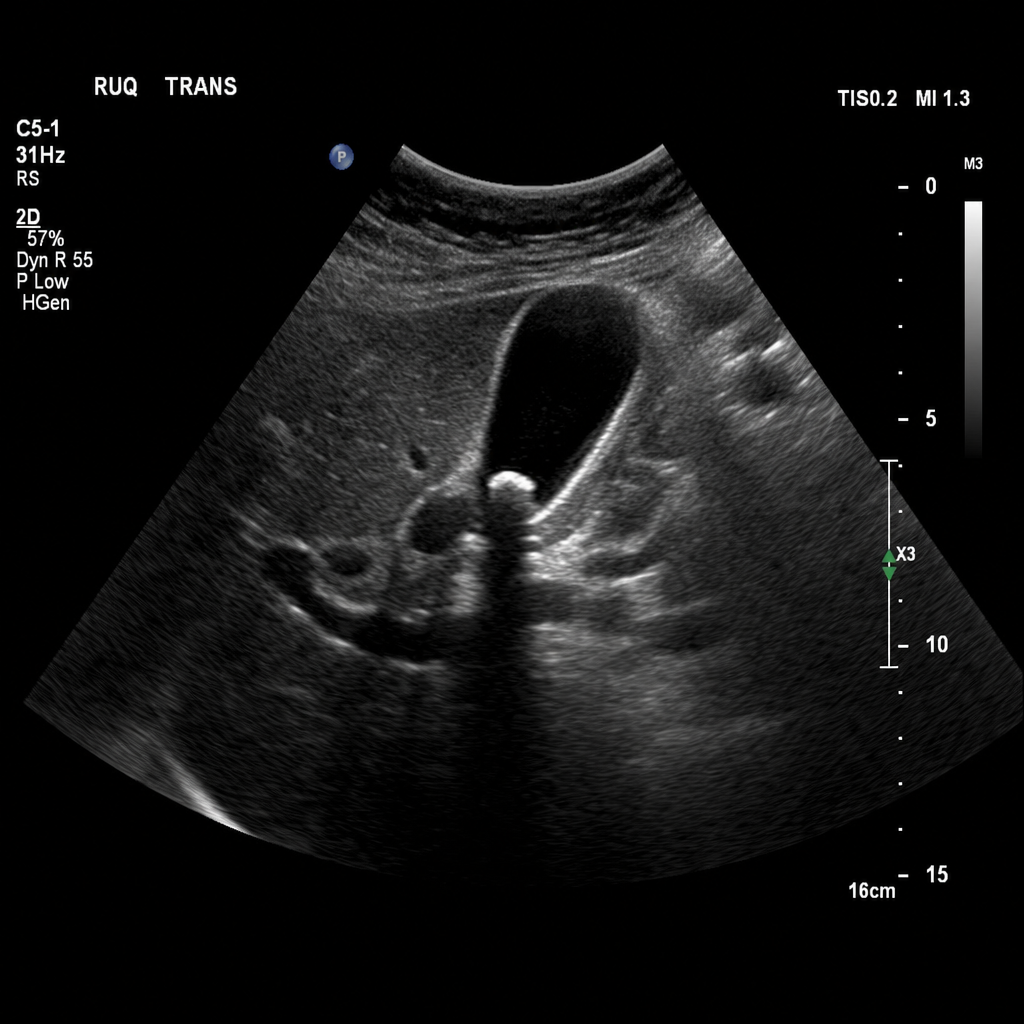
A 43-year-old Caucasian woman is admitted to the hospital with acute onset right upper quadrant (RUQ) pain. The pain started 6 hours ago after the patient had a large meal at a birthday party and has progressively worsened. She recalls having similar pain before but not so intense. No significant past medical history. Current medications are only oral contraceptive. Vitals are blood pressure 140/80 mm Hg, heart rate 79/min, respiratory rate 14/min, and temperature 37.6℃ (99.7℉). The patient's BMI is 36.3 kg/m2. On exam, the patient appears slightly jaundiced. Her cardiac and respiratory examinations are within normal limits. Abdominal palpation reveals tenderness to palpation in the RUQ with no rebound or guarding, and there is an inspiratory arrest on deep palpation in this region. The remainder of the examination is within normal limits. Laboratory tests are significant for the following: RBC count 4.1 million/mm3 Hb 13.4 g/dL Leukocyte count 11,200/mm3 ESR 22 mm/hr Platelet count 230,000/mm3 Total bilirubin 2 mg/dL Direct bilirubin 1.1 mg/dL ALT 20 IU/L AST 18 IU/L Amylase 33 IU/L Ultrasound of the abdomen shows the following result (see image): The common bile duct (CBD) (not shown in the image) is not dilated, and the ultrasound demonstrates gallbladder wall thickening and pericholecystic fluid consistent with acute cholecystitis. Which of the following procedures is most appropriate for the treatment of this patient?
Practice by Chapter
Liver Anatomy and Physiology
Practice Questions
Benign Liver Lesions
Practice Questions
Liver Abscess
Practice Questions
Hepatocellular Carcinoma
Practice Questions
Metastatic Liver Disease
Practice Questions
Cirrhosis and Portal Hypertension
Practice Questions
Liver Trauma
Practice Questions
Cholelithiasis and Cholecystitis
Practice Questions
Choledocholithiasis
Practice Questions
Biliary Tract Tumors
Practice Questions
ERCP and Its Complications
Practice Questions
Liver Transplantation Basics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app