
Hepatobiliary Surgery — MCQs

On this page
Which of the following is the classical triad of acute cholangitis?
A 55-year-old diabetic male develops sudden-onset severe abdominal pain 3 days after an uncomplicated laparoscopic cholecystectomy. Examination reveals peritonitis with guarding and rigidity. Abdominal X-ray shows free air under the diaphragm. What is the most likely diagnosis?
Identify the instrument in the image:

A splenorenal shunt procedure may be required for treatment of:
A 25-year-old shepherd presents with dragging discomfort in right hypochondrium and on examination shows presence of enlarged liver 5 cm below costal margins. The probable diagnosis is:
A 20-year-old patient presents with fever and tenderness in RUQ. CT abdomen shows a lesion measuring 10 cm × 4 cm. Which is the preferred site for aspiration?
Which classification is used to evaluate the condition shown in the image below?

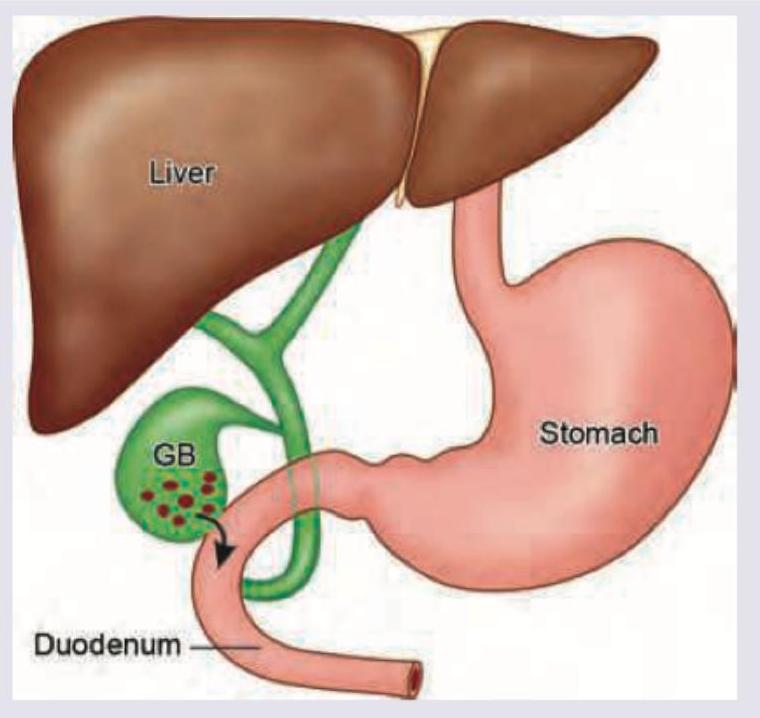
A patient with chronic cholelithiasis develops the complication shown in the image below. This leads to development of:
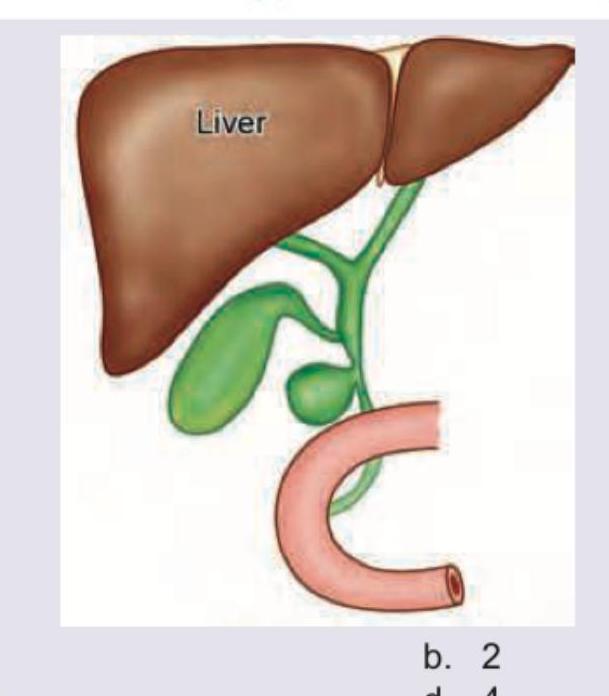
What type of choledochal cyst is shown in the image?
The image shows: (DNB Pattern 2018)

Practice by Chapter
Liver Anatomy and Physiology
Practice Questions
Benign Liver Lesions
Practice Questions
Liver Abscess
Practice Questions
Hepatocellular Carcinoma
Practice Questions
Metastatic Liver Disease
Practice Questions
Cirrhosis and Portal Hypertension
Practice Questions
Liver Trauma
Practice Questions
Cholelithiasis and Cholecystitis
Practice Questions
Choledocholithiasis
Practice Questions
Biliary Tract Tumors
Practice Questions
ERCP and Its Complications
Practice Questions
Liver Transplantation Basics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app