
Hepatobiliary Surgery — MCQs

On this page
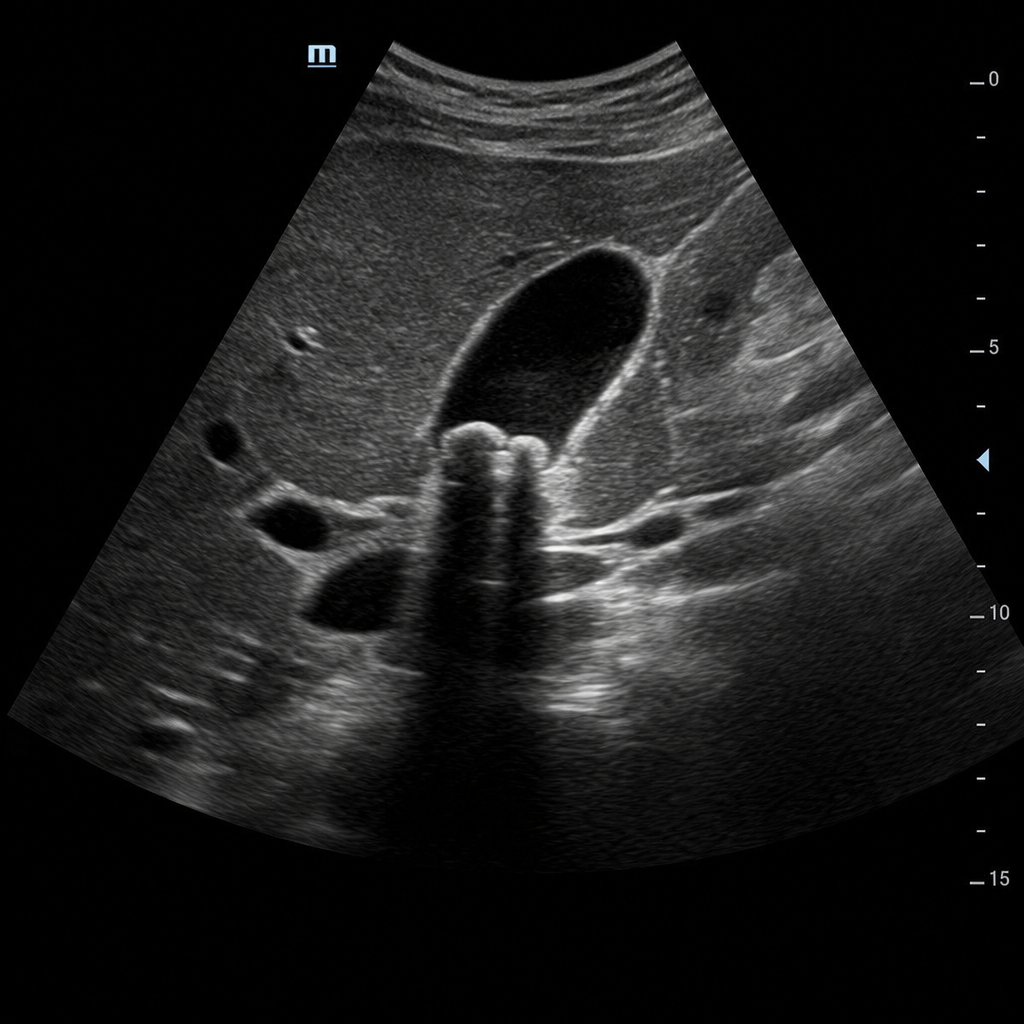
A 30-year-old patient complains of abdominal pain for 5 days, with a similar history in the recent past. On examination, localized tenderness in the right upper quadrant on deep palpation is observed, along with slight yellowish discoloration of the skin. Laboratory tests reveal elevated Alkaline Phosphatase and conjugated bilirubin. Ultrasonography reveals certain findings, including a dilated common bile duct (>6 mm). If this patient had associated gallstones, which of the following would be the most likely diagnosis?
A patient with cholangitis underwent surgical intervention. The investigation shown in the post-operative period on the 10th day is:

A patient with cholangitis underwent surgical intervention. The investigation shown in the post-operative period on the 10th day is:

Which of the following statements about cholangiocarcinoma is false?
Which of the following statements about gall stones is true?
Which of the following is FALSE regarding hepatic adenoma?
Which of the following clinical situations is associated with an increase in predominantly conjugated ("direct") bilirubin?
What is the most common complication after ERCP?
A 30-year-old female presented with pain in the right upper quadrant of the abdomen after 4 days of cholecystectomy. On USG, it showed a significant collection in RUQ. What will you do further?
A 46-year-old male had a tumor in his left lobe of liver, so left sided hemi hepatectomy was planned. Which of the following segments of the liver will be resected in this procedure?
Practice by Chapter
Liver Anatomy and Physiology
Practice Questions
Benign Liver Lesions
Practice Questions
Liver Abscess
Practice Questions
Hepatocellular Carcinoma
Practice Questions
Metastatic Liver Disease
Practice Questions
Cirrhosis and Portal Hypertension
Practice Questions
Liver Trauma
Practice Questions
Cholelithiasis and Cholecystitis
Practice Questions
Choledocholithiasis
Practice Questions
Biliary Tract Tumors
Practice Questions
ERCP and Its Complications
Practice Questions
Liver Transplantation Basics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app