
Hepatobiliary Surgery — MCQs

On this page
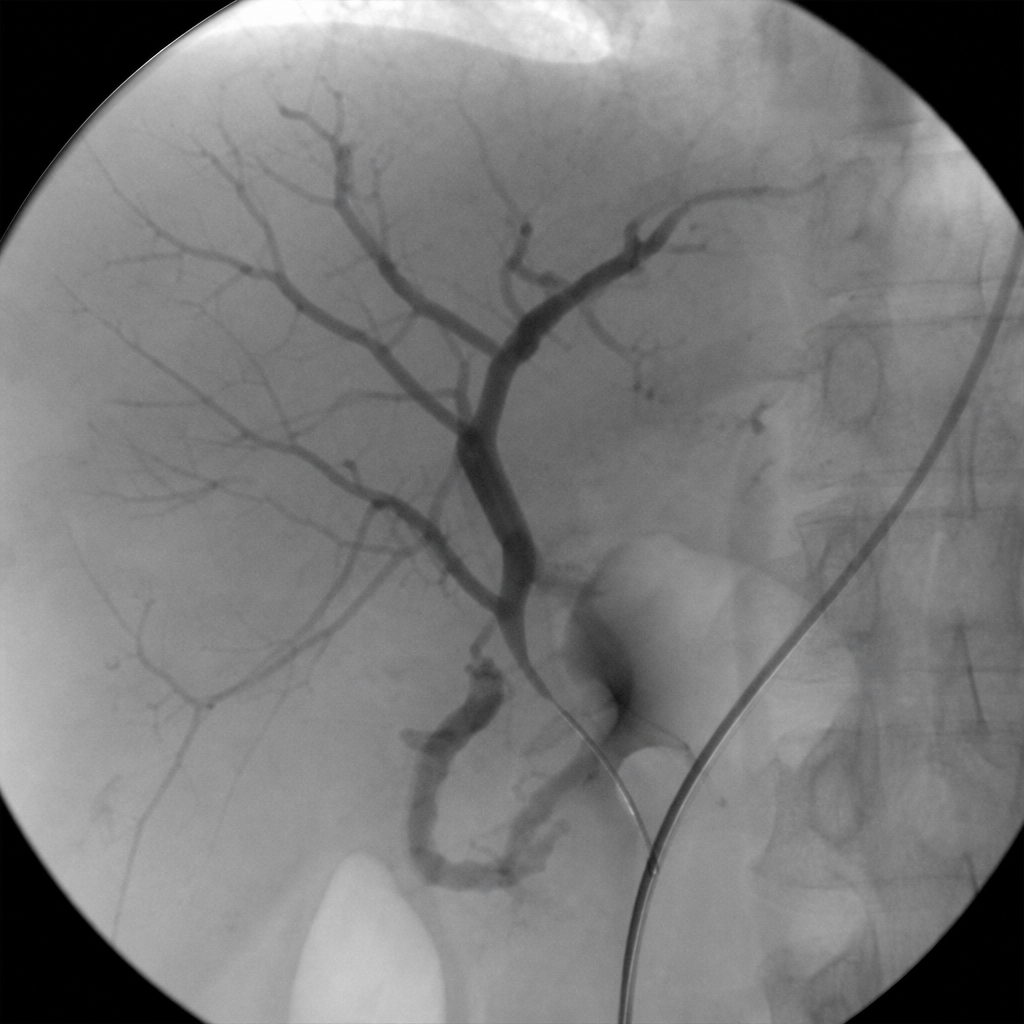
The image below shows a distal splenorenal (Warren) shunt. What is the type of this shunt?
Which of the following is NOT true of cholelithiasis?
All of the following are associated with Caroli's disease, EXCEPT:
All are indicators of active bleeding from varices during endoscopy, EXCEPT:
Bile strictures are most commonly seen in which of the following conditions?
What is the investigation of choice for choledochal cyst?
Mirizzi syndrome is characterized by all the following except:
Which part of the intrahepatic bile duct is involved in Type 2 cholangiocarcinoma?
Which of the following is the least common presentation of Hepatocellular Carcinoma (HCC)?
What is the recommended timing for performing cholangiography with a T-tube after cholecystectomy?
Practice by Chapter
Liver Anatomy and Physiology
Practice Questions
Benign Liver Lesions
Practice Questions
Liver Abscess
Practice Questions
Hepatocellular Carcinoma
Practice Questions
Metastatic Liver Disease
Practice Questions
Cirrhosis and Portal Hypertension
Practice Questions
Liver Trauma
Practice Questions
Cholelithiasis and Cholecystitis
Practice Questions
Choledocholithiasis
Practice Questions
Biliary Tract Tumors
Practice Questions
ERCP and Its Complications
Practice Questions
Liver Transplantation Basics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app