
Hepatobiliary Surgery — MCQs

On this page
All of the following are modalities of therapy for hepatocellular carcinoma except?
Which of the following is NOT an indication for cholecystectomy for gallstone disease?
Which tumor marker is most frequently elevated in carcinoma of the gall bladder?
Which of the following is NOT a risk factor for cholangiocarcinoma?
Which of the following is NOT an indication for cholecystectomy?
A patient with a history of choledocholithiasis presents with elevated conjugated bilirubin. Ultrasound reveals a dilated biliary system up to the terminal part. In case of suspicion of an ampullary obstructive calculus, which of the following investigations would be most sensitive?
Liver tunneling procedures are not performed for which segment?
Five days after common bile duct surgery, a small leak is detected. What is the most appropriate treatment?
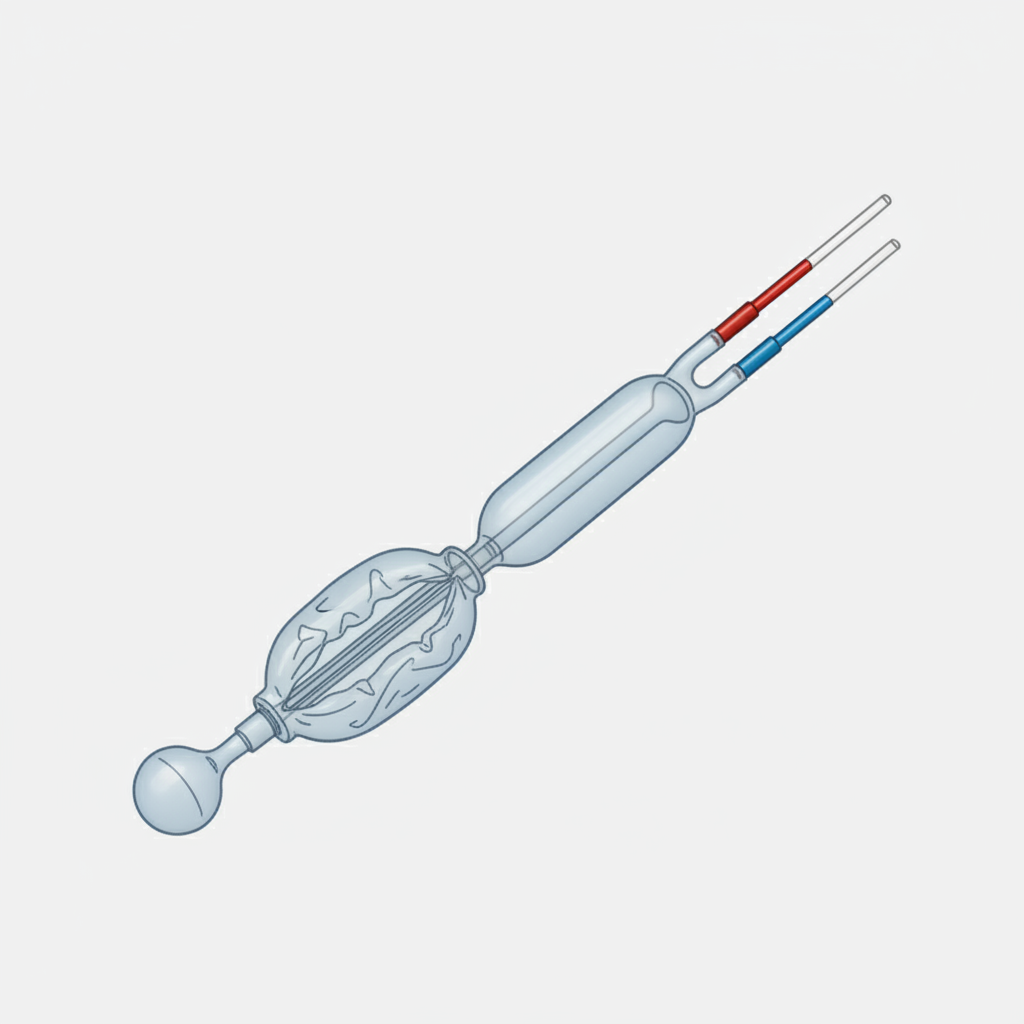
The below instrument is used for the treatment of:
Formation of gall stones occurs in all EXCEPT?
Practice by Chapter
Liver Anatomy and Physiology
Practice Questions
Benign Liver Lesions
Practice Questions
Liver Abscess
Practice Questions
Hepatocellular Carcinoma
Practice Questions
Metastatic Liver Disease
Practice Questions
Cirrhosis and Portal Hypertension
Practice Questions
Liver Trauma
Practice Questions
Cholelithiasis and Cholecystitis
Practice Questions
Choledocholithiasis
Practice Questions
Biliary Tract Tumors
Practice Questions
ERCP and Its Complications
Practice Questions
Liver Transplantation Basics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app