
Hepatobiliary Surgery — MCQs

On this page
Which of the following is a characteristic feature of periampullary carcinoma?
Bleeding adjacent to the Triangle of Calot should be controlled by which method?
A 60-year-old woman, recovering from major pelvic cancer surgery, develops severe abdominal pain and sepsis. Following a positive HIDA scan, laparotomy is performed. The gallbladder is found to be severely inflamed and removed. There is no evidence of gallbladder stones. Which of the following is true regarding acalculous cholecystitis?
Which of the following tumors is typically found incidentally during investigations?
Which of the following is not a major high-risk factor for cholangiocarcinoma?
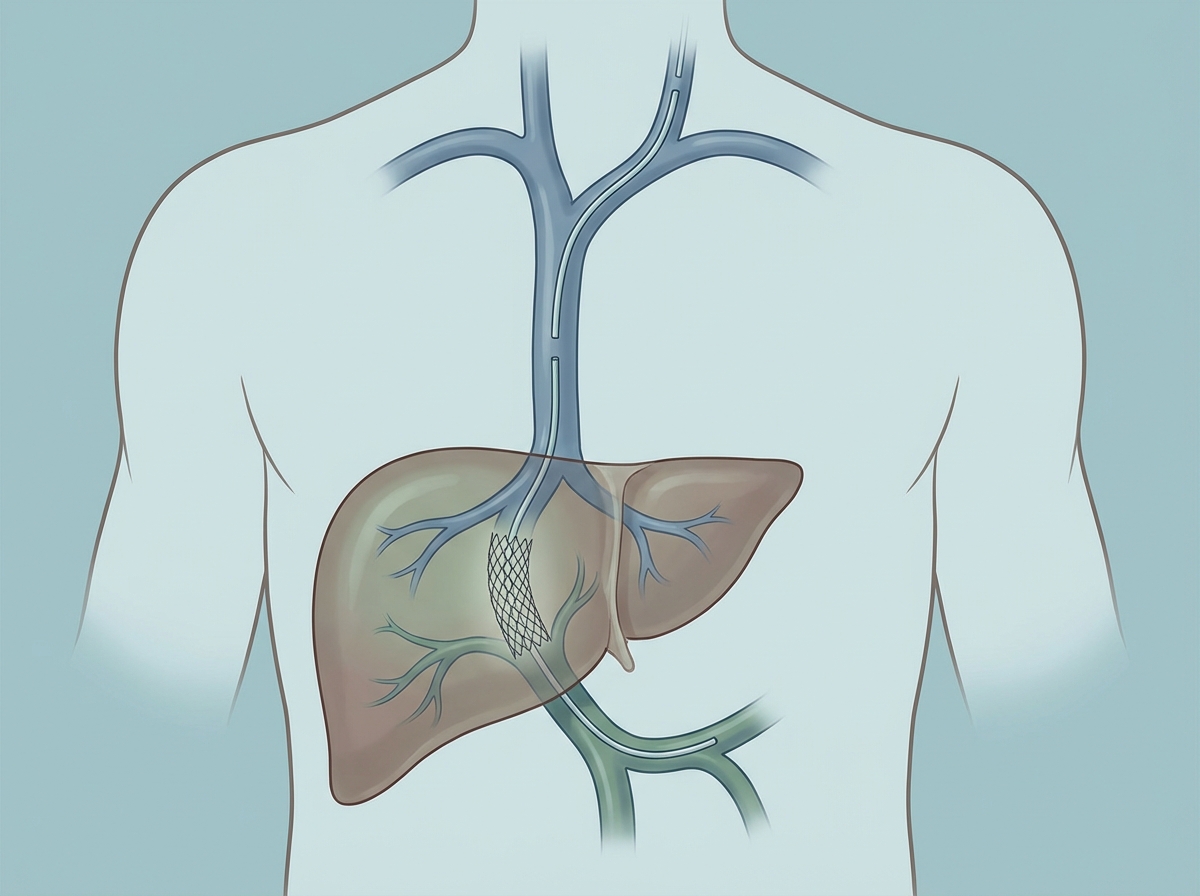
Following placement of a covered-stent TIPS, which of the following is the most common early clinical complication of this procedure?
Increased risk of hepatic malignancy is seen in which benign liver tumor?
What incision approach is used for a mesocaval shunt?
Which of the following originates at the hilum of the liver?
All of the following are known predisposing factors for cholangiocarcinoma except:
Practice by Chapter
Liver Anatomy and Physiology
Practice Questions
Benign Liver Lesions
Practice Questions
Liver Abscess
Practice Questions
Hepatocellular Carcinoma
Practice Questions
Metastatic Liver Disease
Practice Questions
Cirrhosis and Portal Hypertension
Practice Questions
Liver Trauma
Practice Questions
Cholelithiasis and Cholecystitis
Practice Questions
Choledocholithiasis
Practice Questions
Biliary Tract Tumors
Practice Questions
ERCP and Its Complications
Practice Questions
Liver Transplantation Basics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app