
Hepatobiliary Surgery — MCQs

On this page
For bleeding varices of the esophagus, which operation or operations are commonly performed?
Which of the following complications can arise from gallstones?
What is the most important hepatic function to consider after hepatic resection?
Which of the following is a non-selective shunt?
Which of the following is included in the Chilaiditi's sign criteria?
Bile duct injury is detected after 72 hours of surgery. What is the treatment option?
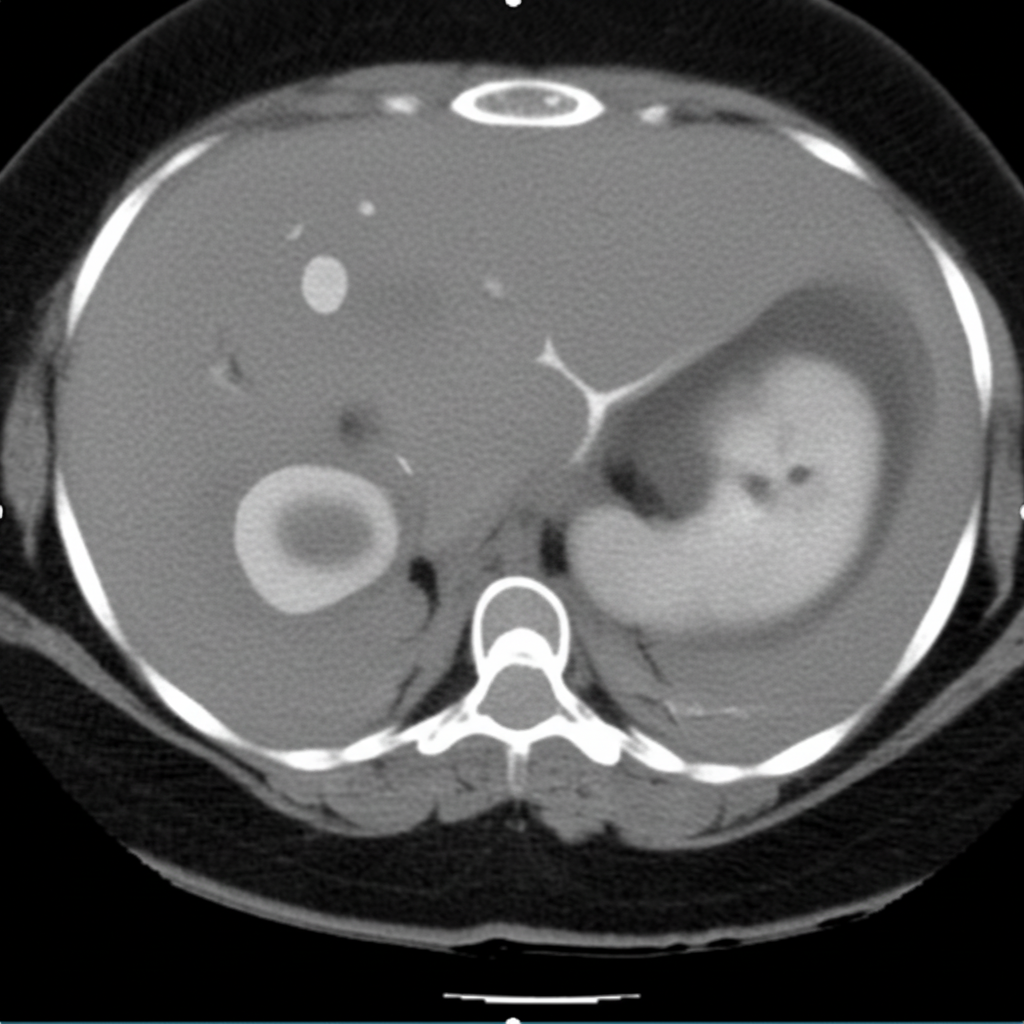
A 35-year-old man presents with right upper quadrant pain and fever. He recently returned from a trip to an endemic area. Aspiration of the lesion seen on the CT image yields thick, reddish-brown fluid. What is the most likely diagnosis?
What is the preferred shunt procedure in a patient with portal hypertension who has acceptable operative risk and adequate liver function?
In which stage of gallbladder carcinoma is liver lobe resection considered for patients with carcinoma of the gallbladder?
A patient with an 8 cm x 8 cm abscess in the right lobe of the liver was treated with multiple aspirations (3 times) and systemic amebicides. A cavity remains in the right lobe of the liver, but it is now empty. A seven-day course of luminal amebicides has been administered. How will you follow up?
Practice by Chapter
Liver Anatomy and Physiology
Practice Questions
Benign Liver Lesions
Practice Questions
Liver Abscess
Practice Questions
Hepatocellular Carcinoma
Practice Questions
Metastatic Liver Disease
Practice Questions
Cirrhosis and Portal Hypertension
Practice Questions
Liver Trauma
Practice Questions
Cholelithiasis and Cholecystitis
Practice Questions
Choledocholithiasis
Practice Questions
Biliary Tract Tumors
Practice Questions
ERCP and Its Complications
Practice Questions
Liver Transplantation Basics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app