
Hepatobiliary Surgery — MCQs

On this page
An 85-year-old man presents with a 2-day history of nausea and vomiting. He has not passed gas or moved his bowels for the last 5 days. Abdominal films show dilated small bowel, no air in the rectum, and air in the biliary tree. Which of the following statements is true?
Which of the following is NOT a feature of choledocholithiasis?
A patient with compensated liver cirrhosis presented with a history of variceal bleed. What is the preferred mode of treatment in this patient?
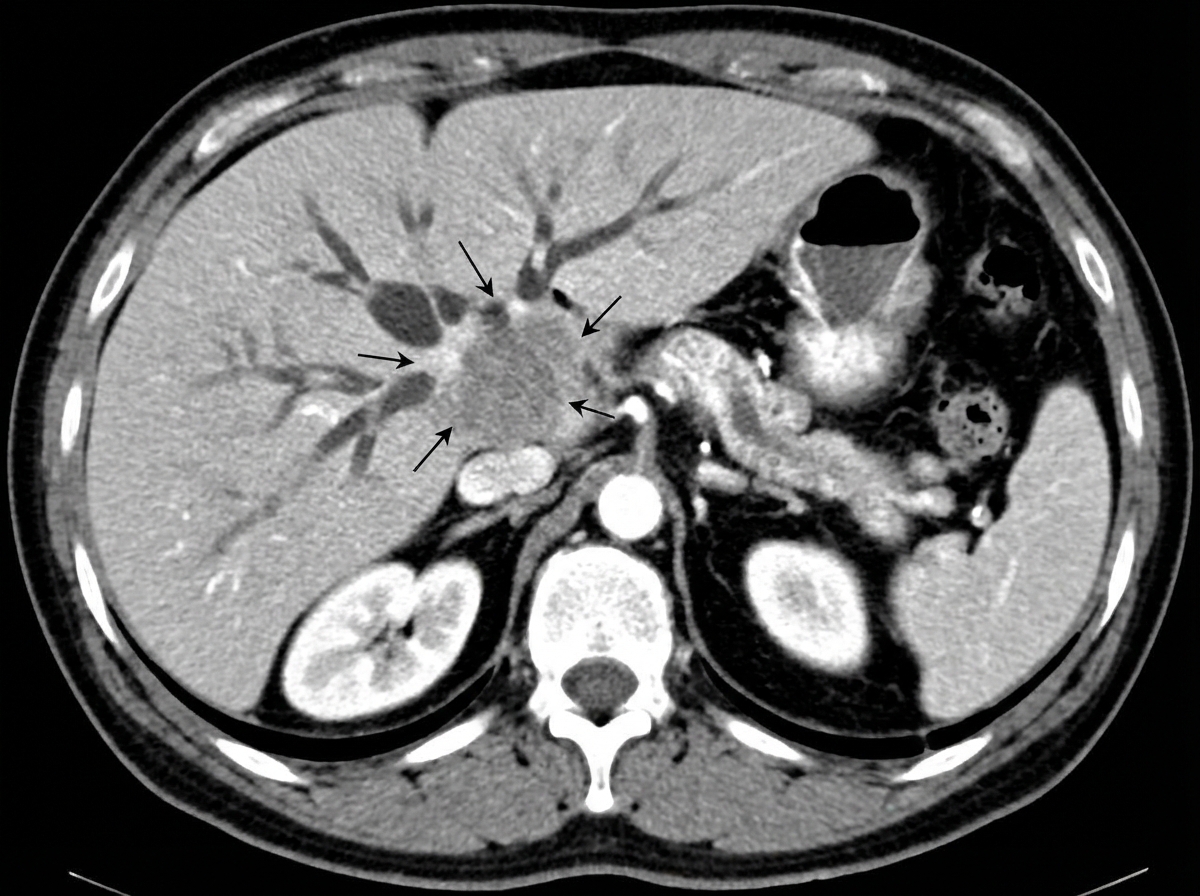
A 70-year-old male presented with progressive jaundice for 6 weeks, fever, pruritis along with abdominal pain and significant weight loss. Lab findings reveal total serum bilirubin of 22 mg/dL, minimally elevated SGOT/SGPT, and increased alkaline phosphatase. A CT abdomen and ERCP were performed. What is the most common site of this pathology?
Which of the following are included in the Child criteria?
A 50-year-old man presents with a one-week history of fever and abdominal pain. An abdominal ultrasound revealed a hypoechoic liver lesion, and a CECT was performed for characterization. Which of the following statements regarding the lesion is false?
Okuda staging for HCC includes all except?
Which of the following is a criterion for assessing the prognosis of a portosystemic shunt?
What is the ideal treatment for stenosis of the sphincter of Oddi?
All of the following modalities can be used for in situ ablation of liver secondaries, except?
Practice by Chapter
Liver Anatomy and Physiology
Practice Questions
Benign Liver Lesions
Practice Questions
Liver Abscess
Practice Questions
Hepatocellular Carcinoma
Practice Questions
Metastatic Liver Disease
Practice Questions
Cirrhosis and Portal Hypertension
Practice Questions
Liver Trauma
Practice Questions
Cholelithiasis and Cholecystitis
Practice Questions
Choledocholithiasis
Practice Questions
Biliary Tract Tumors
Practice Questions
ERCP and Its Complications
Practice Questions
Liver Transplantation Basics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app