
Hepatobiliary Surgery — MCQs

On this page
Which of the following are considered risk factors for gallstones?
Splenectomy is useful in which of the following conditions?
Which of the following statements regarding carcinoma of the gallbladder is FALSE?
In a patient undergoing right hepatic lobectomy, which of the following are important operative steps?
Which of the following is NOT a complication after endoscopic sclerotherapy?
What is the treatment of choice for an 8 mm retained common bile duct (CBD) stone?
In hemolytic anemia, which type of gallstones are commonly seen?
In which of the following conditions is splenectomy not useful?
Splenectomy is indicated in:
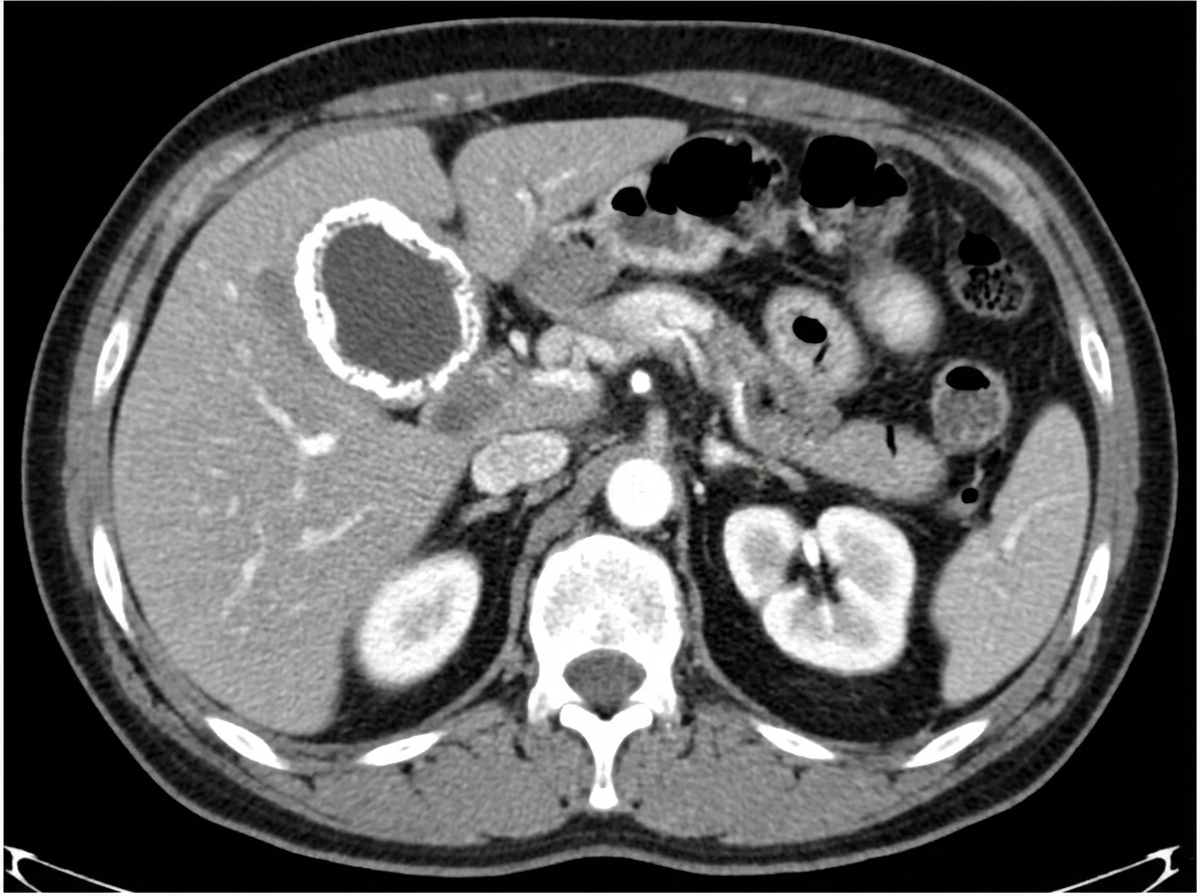
All of the following are true about an incidental finding in a 56-year-old female patient who underwent a CECT abdomen, except?
Practice by Chapter
Liver Anatomy and Physiology
Practice Questions
Benign Liver Lesions
Practice Questions
Liver Abscess
Practice Questions
Hepatocellular Carcinoma
Practice Questions
Metastatic Liver Disease
Practice Questions
Cirrhosis and Portal Hypertension
Practice Questions
Liver Trauma
Practice Questions
Cholelithiasis and Cholecystitis
Practice Questions
Choledocholithiasis
Practice Questions
Biliary Tract Tumors
Practice Questions
ERCP and Its Complications
Practice Questions
Liver Transplantation Basics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app