
Hepatobiliary Surgery — MCQs

On this page
During a laparoscopic cholecystectomy, a lateral injury to the Common Bile Duct is identified. What is the most appropriate next step in management?
A 60-year-old patient presents with pruritus and obstructive jaundice. Physical examination reveals a palpable, non-tender gallbladder. What is the most likely diagnosis?
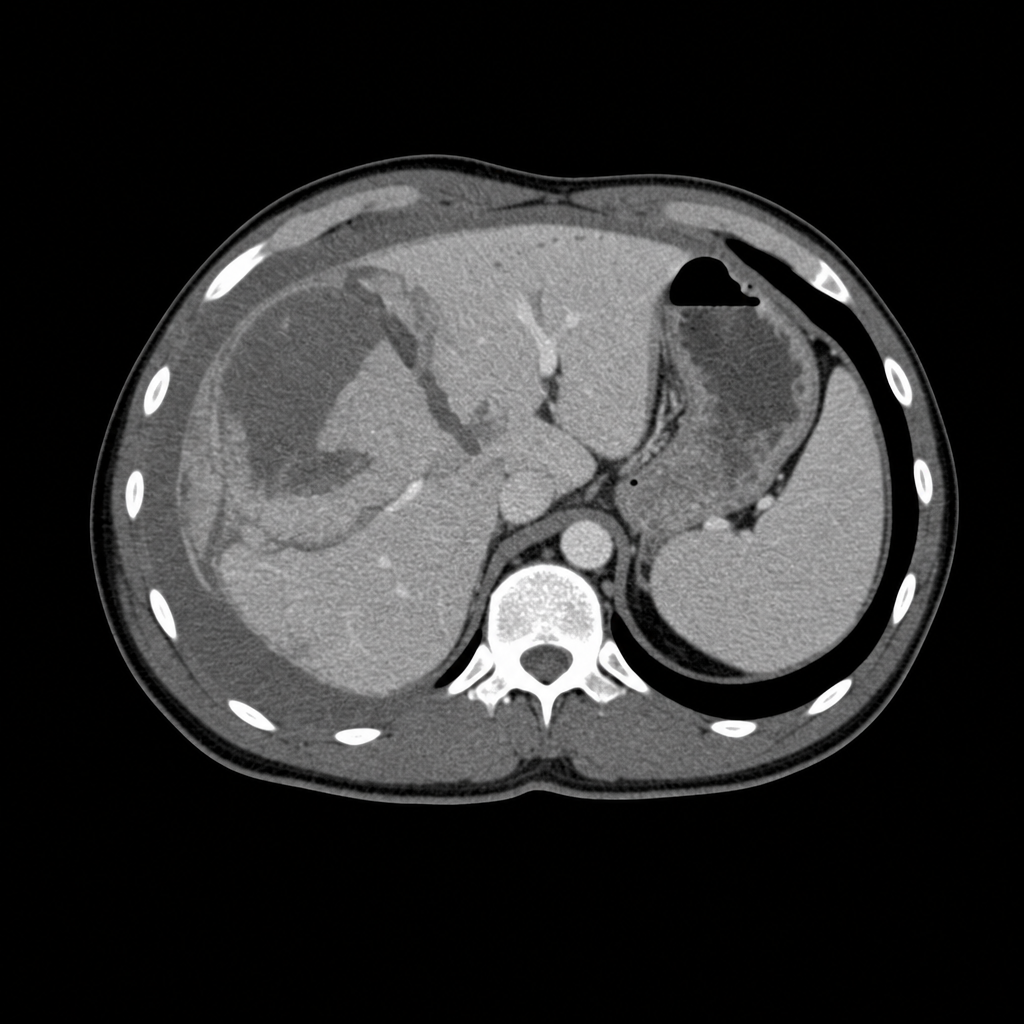
A 28-year-old unrestrained male driver is brought to the trauma bay following a high-speed road traffic collision. Primary survey: GCS 14, HR 118 bpm, BP 94/60 mmHg with partial response to 1 litre of crystalloid. FAST examination is positive in the right upper quadrant. After partial haemodynamic stabilisation, a CT abdomen with contrast is performed and is shown (Image 2). His BP on return from CT is 88/54 mmHg despite ongoing resuscitation. What is the most appropriate next step?
What organism causes emphysematous cholecystitis?
Klatskin tumor is defined as:
What condition is characterized by a "crumbled egg appearance" in the liver?
Which of the following is NOT a part of the management of a stone in the common bile duct?
Which of the following statements regarding Hepatocellular Carcinoma (HCC) is true?
A forty-year-old female visits the hospital with a complaint of pain in her right hypochondriac region radiating towards the right shoulder tip. The pain begins after eating food and increases steadily over 10-30 minutes, then gradually decreases. What condition might she have?
What is the most common association seen in gallbladder carcinoma?
Practice by Chapter
Liver Anatomy and Physiology
Practice Questions
Benign Liver Lesions
Practice Questions
Liver Abscess
Practice Questions
Hepatocellular Carcinoma
Practice Questions
Metastatic Liver Disease
Practice Questions
Cirrhosis and Portal Hypertension
Practice Questions
Liver Trauma
Practice Questions
Cholelithiasis and Cholecystitis
Practice Questions
Choledocholithiasis
Practice Questions
Biliary Tract Tumors
Practice Questions
ERCP and Its Complications
Practice Questions
Liver Transplantation Basics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app