
Head and Neck Surgery — MCQs

On this page
Which surgical landmarks are used for locating the facial nerve?
A 23-year-old male patient presents with midline swelling in the neck. The swelling moves with deglutition and protrusion of the tongue. What is the likely diagnosis?
A middle-aged man presents with a swelling in the neck that has been present since childhood. The swelling has a bag or worm-like appearance and features a central black spot. Based on this description, what is the most likely diagnosis?
What is Pott’s puffy tumor?
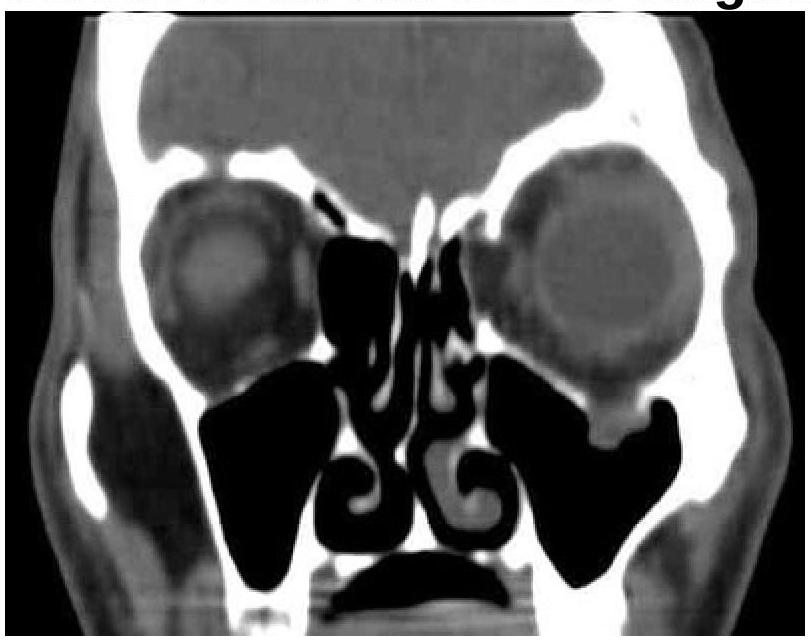
A patient presented with a history of diplopia and restricted eye movements. What is the most likely diagnosis based on the clinical and CT images?
In which condition is surgical intervention involving partial or full closure of the nasal cavity typically performed?
What is the most common cause of a parotid mass that presents with mixed consistency?
Where will be the placement location for Auditory Brainstem Implant?
Which of the following stages of lip carcinoma does not have nodal involvement?
Which of the following statements about Branchial cysts is true:
Practice by Chapter
Salivary Gland Diseases
Practice Questions
Thyroid Gland Disorders
Practice Questions
Parathyroid Gland Disorders
Practice Questions
Neck Masses Evaluation
Practice Questions
Oral Cavity Lesions
Practice Questions
Laryngeal Disorders
Practice Questions
Head and Neck Cancer
Practice Questions
Reconstructive Techniques in Head and Neck Surgery
Practice Questions
Surgical Management of Sleep Apnea
Practice Questions
Airway Management in Head and Neck Surgery
Practice Questions
Surgical Approaches to the Neck
Practice Questions
Neck Dissection Techniques
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app