
Head and Neck Surgery — MCQs

On this page
A 35-year-old lady who presented with a 6-month painless fluctuant, non-transilluminant swelling with a thin watery discharge. Clinical diagnosis is?
What is the most likely diagnosis for this 60-year-old man with the lesion shown in the image?

Investigations used for CSF rhinorrhea are all except:
A 46-year-old patient develops a verrucous carcinoma in the oral cavity. What is true of this lesion?
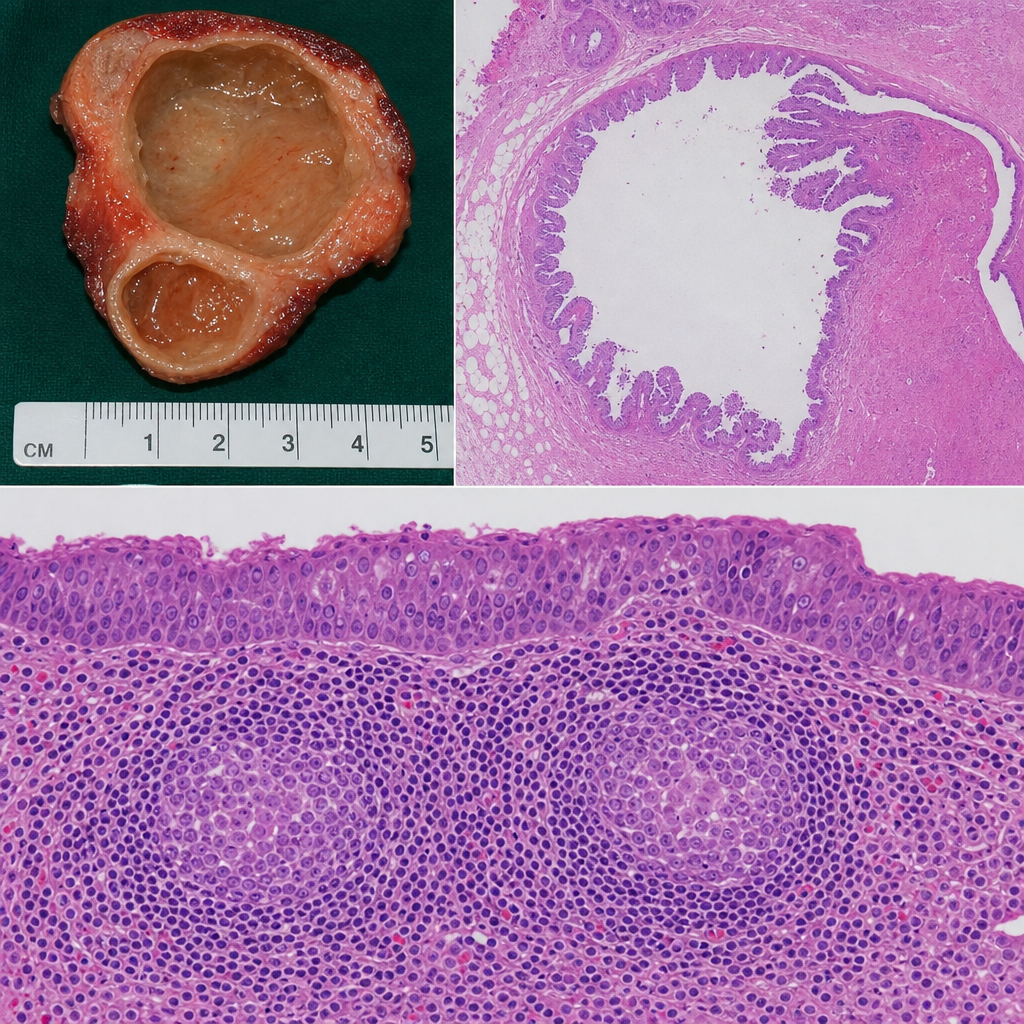
While shaving, a 45-year-old teacher notices a marble-sized mass beneath his left ear. The mass is eventually excised, revealing which of the following benign parotid gland lesions?
Best method to evaluate bone defect is
Which cancer has maximum propensity to spread to cervical lymph nodes?
Carcinoma tongue less than 2 cm is treated by -
Which of the following is false about parotid tumor
N3a TNM staging of head and neck tumors (AJCC 8th edition) shows:
Practice by Chapter
Salivary Gland Diseases
Practice Questions
Thyroid Gland Disorders
Practice Questions
Parathyroid Gland Disorders
Practice Questions
Neck Masses Evaluation
Practice Questions
Oral Cavity Lesions
Practice Questions
Laryngeal Disorders
Practice Questions
Head and Neck Cancer
Practice Questions
Reconstructive Techniques in Head and Neck Surgery
Practice Questions
Surgical Management of Sleep Apnea
Practice Questions
Airway Management in Head and Neck Surgery
Practice Questions
Surgical Approaches to the Neck
Practice Questions
Neck Dissection Techniques
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app