
Head and Neck Surgery — MCQs

On this page
A gentleman of 60 years presented with a brawny swelling of the submandibular region with inflammatory edema of mouth and putrid halitosis. Most likely he is suffering from
Tongue fixation in a patient with carcinoma tongue is staged as
Which one of the following structures is not removed during a classical radical neck dissection?
A patient operated for a parotid gland tumour developed symptoms of sweating and erythema (flushing) over the region of surgical excision while eating. The probable diagnosis is:
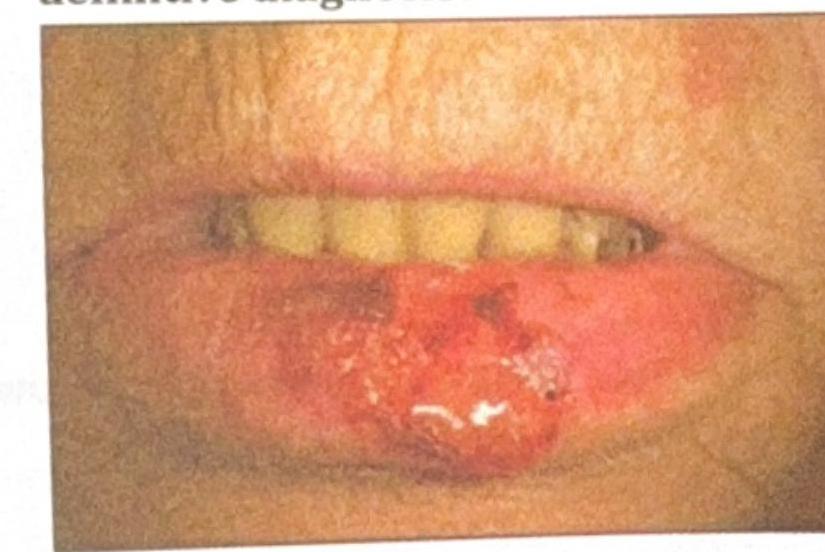
An elderly patient presents with a non-healing ulcerative lesion on the lower lip, as shown in the image. The lesion measures approximately 3 cm in diameter, involves the vermilion border, and extends into the surrounding labial skin, making complete primary excision likely to cause significant cosmetic and functional deformity. The lesion has been gradually enlarging over the past few months. Suspecting squamous cell carcinoma (SCC), what is the most appropriate method to obtain a biopsy for definitive diagnosis?
Which of these is the STRONGEST indication for giving adjuvant treatment in oral malignancy after resection and Modified Radical Neck Dissection (MRND)?
Which nerve is most commonly injured during submandibular gland surgery?
A 35-year-old male presents with posterior epistaxis. Conservative management including nasal packing to stop the bleeding was unsuccessful. What is the next step in the management of this patient?
What is the likely diagnosis of the image given below?

What is the most likely diagnosis for the swelling in the floor of the mouth shown in the image?

Practice by Chapter
Salivary Gland Diseases
Practice Questions
Thyroid Gland Disorders
Practice Questions
Parathyroid Gland Disorders
Practice Questions
Neck Masses Evaluation
Practice Questions
Oral Cavity Lesions
Practice Questions
Laryngeal Disorders
Practice Questions
Head and Neck Cancer
Practice Questions
Reconstructive Techniques in Head and Neck Surgery
Practice Questions
Surgical Management of Sleep Apnea
Practice Questions
Airway Management in Head and Neck Surgery
Practice Questions
Surgical Approaches to the Neck
Practice Questions
Neck Dissection Techniques
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app