
Head and Neck Surgery — MCQs

On this page
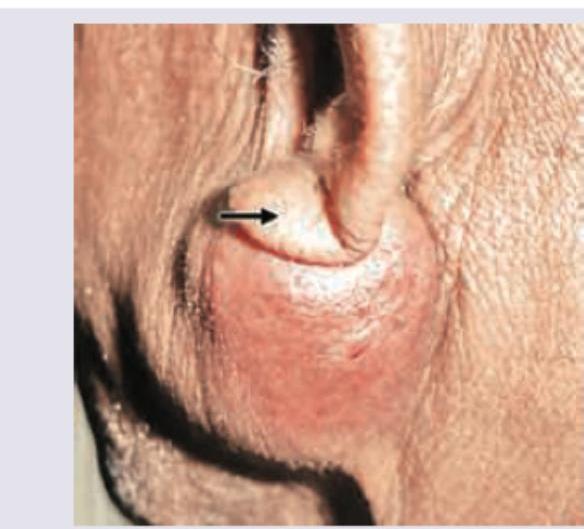
A 45-year-old patient presents with a slowly progressive, painless swelling in the parotid region as shown in the image. The mass is firm, non-tender, and freely mobile. Identify the most likely diagnosis.
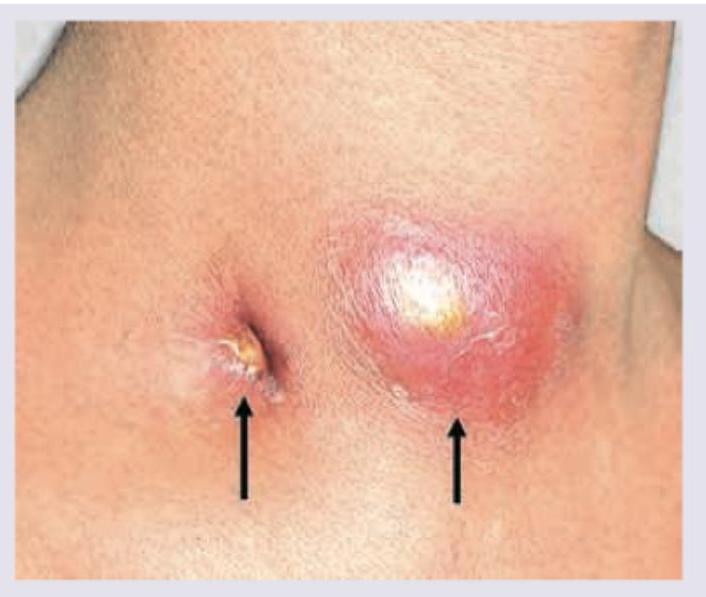
A 35-year-old HIV+ patient presents with the following lesion in the neck. He has been diagnosed with tuberculous cervical lymphadenitis and is currently on ATT. The collection is fluctuant. What is correct about the management?
A 40-year-old smoker presents with soreness of tongue since last 2 months. On examination, it is found that the oral hygiene is poor and there is a white plaque over the lateral border of the tongue. What is the next step in the management of this patient?
The commonest site for thyroglossal cyst is :
The structures removed in radical neck dissection include: 1. Sternocleidomastoid muscle 2. Submandibular gland 3. Internal jugular vein 4. Accessory nerve
Consider the following statements : Branchial cysts : 1. are associated with tracks passing between the carotid bifurcation. 2. usually present in early adulthood. 3. occur along the lower one-third of the anterior border of the sternocleidomastoid muscle. 4. develop from the vestigial remnants of the fourth branchial cleft. Which of the statements given above are correct?
With reference to Le Fort I fracture, consider the following statements : 1. Fracture line separates alveolus and palate from the facial skeleton. 2. Fracture line passes from the pyriform aperture. 3. Fracture line runs posteriorly to include pterygoid plates. 4. Fracture line passes through orbit. Which of the statements given above are correct?
A 50 year old man with long history of swelling in his right parotid region had sudden history of occasional pain, nerve weakness along with paresthesia. His fine needle aspiration cytology was inconclusive. What should be the next step?
In a lateral facial wound, if facial nerve injury is suspected, it should be:
A 70 year old male having comorbidities presents with benign appearing parotid tumour. The best option is:
Practice by Chapter
Salivary Gland Diseases
Practice Questions
Thyroid Gland Disorders
Practice Questions
Parathyroid Gland Disorders
Practice Questions
Neck Masses Evaluation
Practice Questions
Oral Cavity Lesions
Practice Questions
Laryngeal Disorders
Practice Questions
Head and Neck Cancer
Practice Questions
Reconstructive Techniques in Head and Neck Surgery
Practice Questions
Surgical Management of Sleep Apnea
Practice Questions
Airway Management in Head and Neck Surgery
Practice Questions
Surgical Approaches to the Neck
Practice Questions
Neck Dissection Techniques
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app