
Head and Neck Surgery — MCQs

On this page
Swelling of the deep lobe of the parotid gland presents as swelling in which anatomical space?
What surgical approach is indicated for an odontogenic tumor located 1cm from the inferior border of the mandible?
A ranula is most appropriately described by which of the following statements?
All of the following are congenital cysts except?
During extraction of an upper first molar, the mesiobuccal root is missing and is suspected to have been pushed into the maxillary sinus. What is the best immediate patient positioning following this incident?
An 18-year-old male patient presented with pain and swelling in the lower jaw. Intraoral examination revealed localized gingival bleeding in the right posterior region. On palpation, pulsations can be appreciated. Radiographs also showed lesions on the frontal bone. Which condition is present in this patient?
After the parotidectomy operation, a patient presents with excessive sweating and redness over the parotid region. What is the diagnosis?
A 32-year-old patient who is a chronic tobacco chewer presents with a whitish lesion on the gingivobuccal sulcus for 7 months. What is the next best step in the management of this condition?
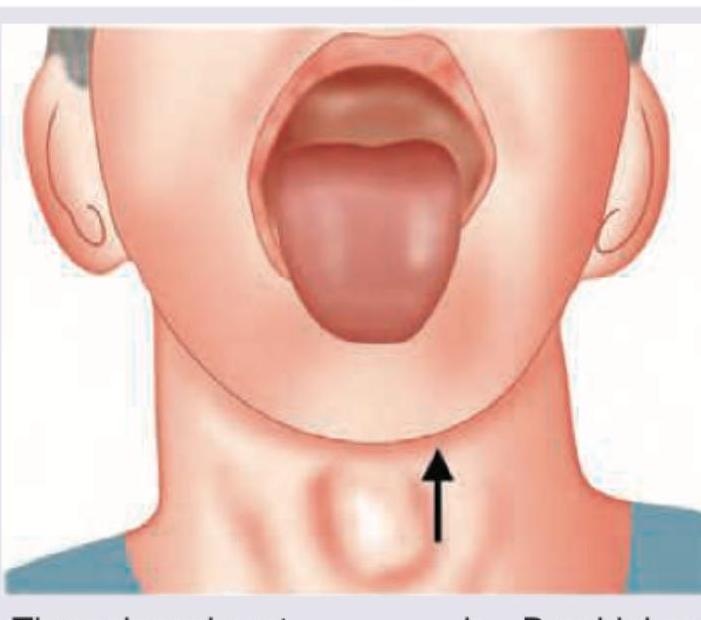
A 22-year-old female patient complains of discharge from the neck along with a previous history of midline neck swelling. Image of the patient is given below. All the statements regarding this patient are true except:

A patient presents with a midline neck mass that moves with swallowing and protrusion of the tongue. The image shows the clinical presentation (arrow indicates the mass). What is the most likely diagnosis?
Practice by Chapter
Salivary Gland Diseases
Practice Questions
Thyroid Gland Disorders
Practice Questions
Parathyroid Gland Disorders
Practice Questions
Neck Masses Evaluation
Practice Questions
Oral Cavity Lesions
Practice Questions
Laryngeal Disorders
Practice Questions
Head and Neck Cancer
Practice Questions
Reconstructive Techniques in Head and Neck Surgery
Practice Questions
Surgical Management of Sleep Apnea
Practice Questions
Airway Management in Head and Neck Surgery
Practice Questions
Surgical Approaches to the Neck
Practice Questions
Neck Dissection Techniques
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app