
Sutures and Stapling Devices — MCQs

Which type of collagen is most abundant in hyaline cartilage?
Which of the following structures in the spermatic cord is typically preserved (not divided) during vasectomy surgery?
For a midline incision in the abdomen, length of suture required is:
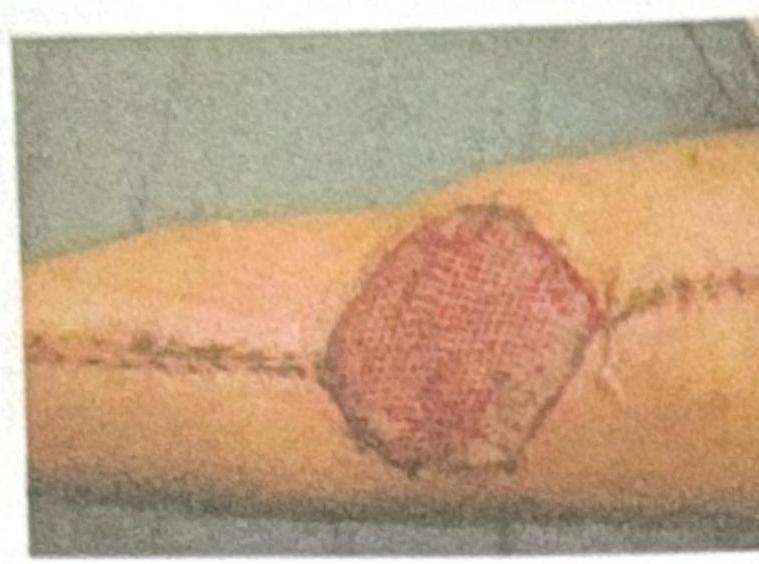
What type of graft or dressing is used to cover the post-burn wound shown in the image?
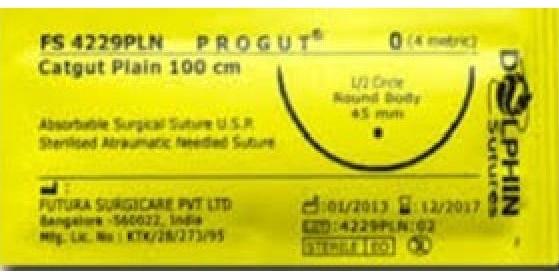
Which of the following statements is true about the suture material shown in the image?
A patient has a lacerated, untidy wound of the leg and attended the casualty department after 2 hours. His wound should be:
Vacuum assisted closure is contraindicated in which of the following conditions -
Which of the following layers are cut during fasciotomy ?
Which one of the following regarding absorbable meshes is NOT true?
What is the typical absorption duration of Polydioxanone sutures?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app