
General Surgery Principles — MCQs

On this page
Multiple air fluid levels in X-ray of abdomen are seen in
Most common cause of acute abdomen in a young girl?
Which nerve is most commonly damaged during hernia repair?
Identify the surgical instrument based on the following characteristics: short blades, sharp cutting edges, and a central screw or rivet. Commonly used for cutting sutures.
Which of the following is not a component of the Thoracoscore?
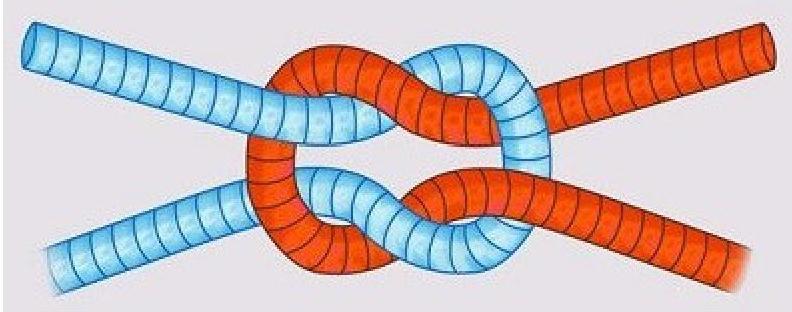
What type of knot is depicted in the image?
A person reports 4 hours after having a clean wound without laceration. He had taken TT 10 years before. The next step in management is:
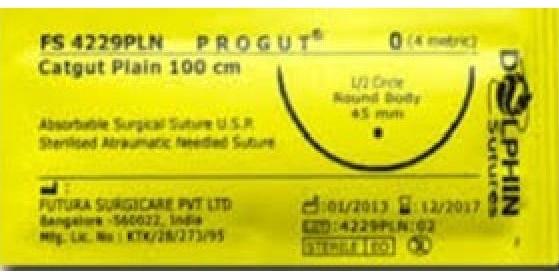
Which of the following statements is true about the suture material shown in the image?
Which of the following layers are cut during fasciotomy ?
Which of the following is a common indication for performing a tracheostomy?
Practice by Chapter
Wound Healing and Care
Practice Questions
Surgical Infections
Practice Questions
Fluid and Electrolyte Management
Practice Questions
Nutrition in Surgical Patients
Practice Questions
Hemostasis and Blood Transfusion
Practice Questions
Surgical Instruments and Equipment
Practice Questions
Sutures and Stapling Devices
Practice Questions
Minimal Access Surgery Principles
Practice Questions
Surgical Complications
Practice Questions
Anesthesia Principles for Surgeons
Practice Questions
Surgical Oncology Principles
Practice Questions
Evidence-Based Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app