
General Surgery Principles — MCQs

On this page
A patient presents with an umbilical mass, which was previously reducible but has now become irreducible with discharge coming out, as shown in the image. What is the most appropriate management?

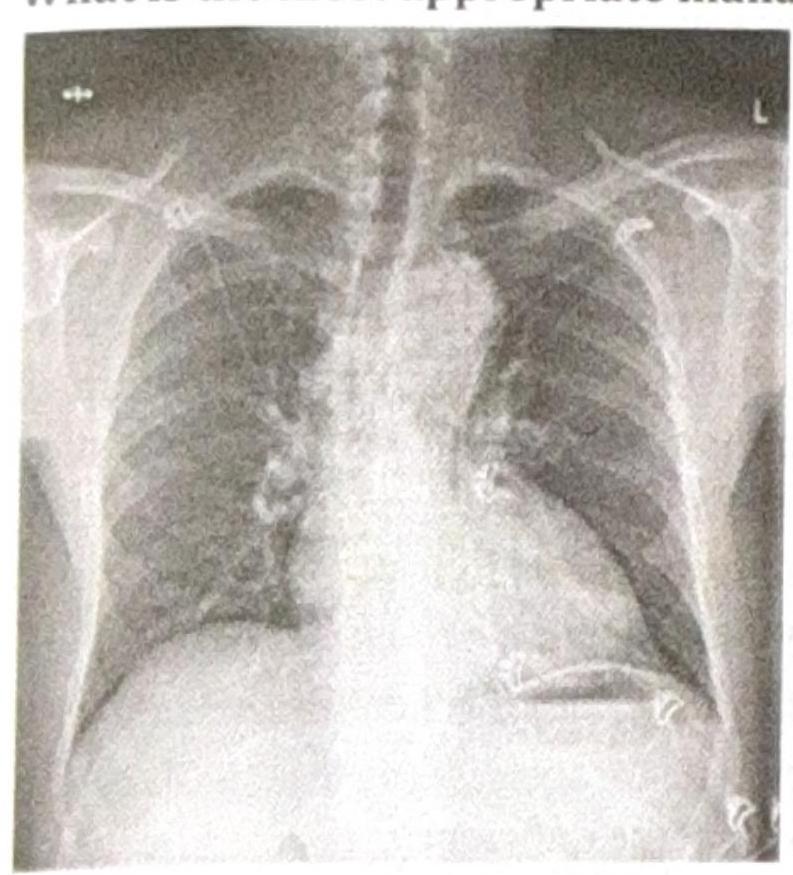
A patient presents with constant chest pain, and the radiological finding is as shown in the image. What is the most appropriate management?
A jeep driver presents with pain in the gluteal region along with swelling and pus discharge for the past 6 months. What is the most likely diagnosis?
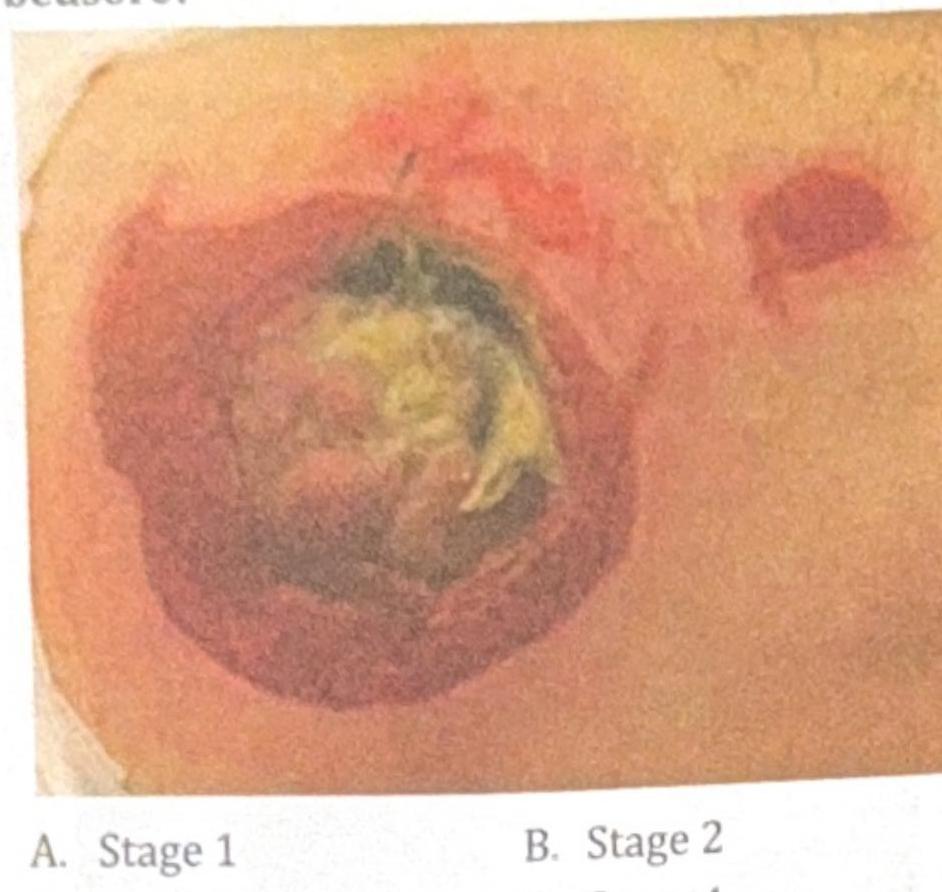
A 78-year-old immobile patient presents with a pressure ulcer on the sacral area, as shown in the image below. How would you grade this bedsore?
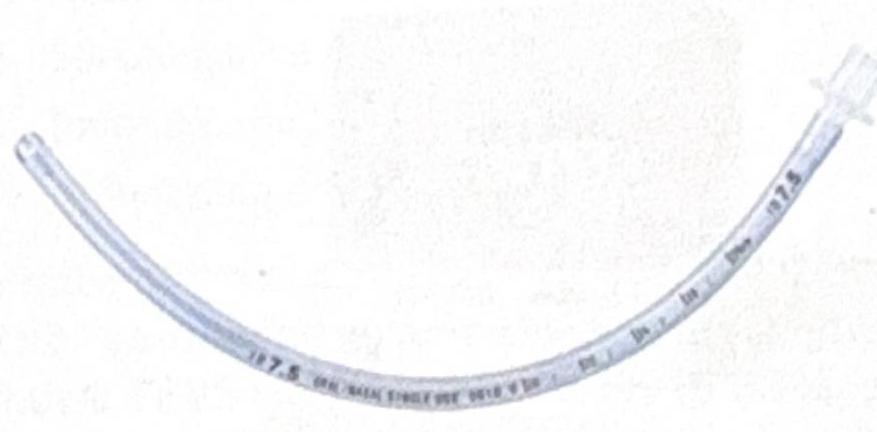
Identify the instrument shown in the image:
In which condition is gas under the diaphragm most commonly seen on imaging?
Which of the following is the most commonly performed repair for a direct inguinal hernia?
Identify the given bone marrow biopsy instrument
A surgeon examined the case of hernia. Forcefully reduces the sac in abdominal cavity, without actually pushing back the contents. Identify the type of hernia.
A surgeon examined a case of hernia and was able to retract the hernial sac on examination but not the contents. Identify the type of hernia depicted in the image.

Practice by Chapter
Wound Healing and Care
Practice Questions
Surgical Infections
Practice Questions
Fluid and Electrolyte Management
Practice Questions
Nutrition in Surgical Patients
Practice Questions
Hemostasis and Blood Transfusion
Practice Questions
Surgical Instruments and Equipment
Practice Questions
Sutures and Stapling Devices
Practice Questions
Minimal Access Surgery Principles
Practice Questions
Surgical Complications
Practice Questions
Anesthesia Principles for Surgeons
Practice Questions
Surgical Oncology Principles
Practice Questions
Evidence-Based Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app