
General Surgery Principles — MCQs

On this page
A surgical suture material is shown in the image below. Which of the following statements is TRUE about this suture?

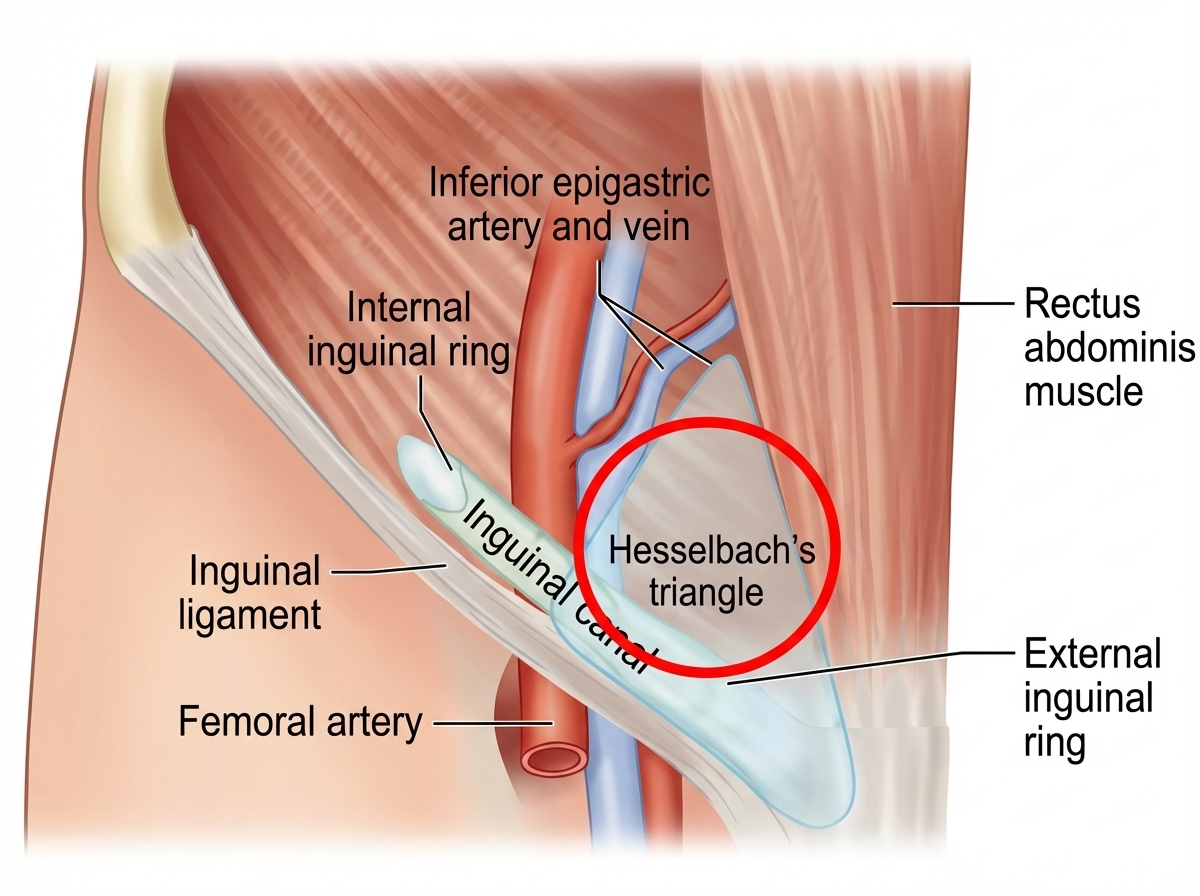
The patient has developed a hernia at the site highlighted by red circle. What is this hernia called as per NYHUS classification? (NEET Pattern 2018)
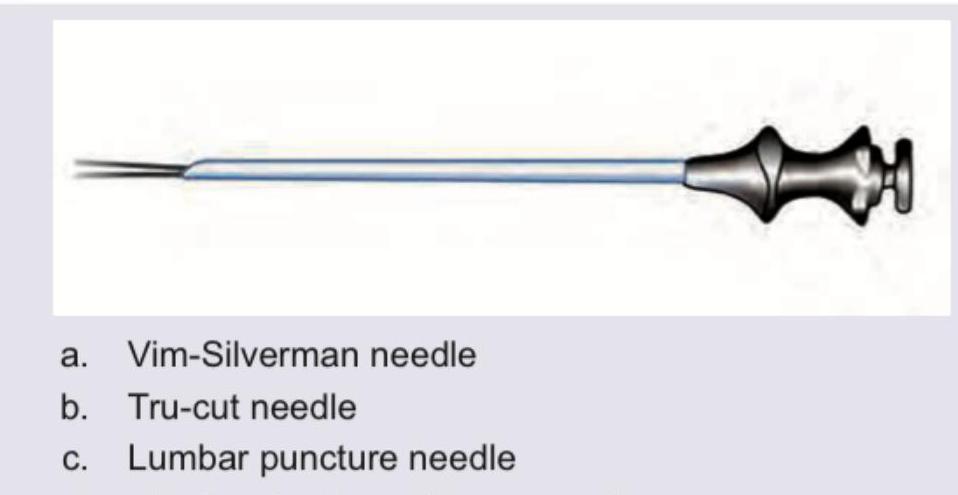
Identify the instrument shown in the image, which is a lumbar puncture needle with a sharp cutting edge and a hub indicating CSF.
A 60-year-old male presents to the emergency department on the second day of symptom onset with progressive deterioration of consciousness due to large right MCA territory infarct. Which of the following is the most appropriate management? (Image: img-179.jpeg)
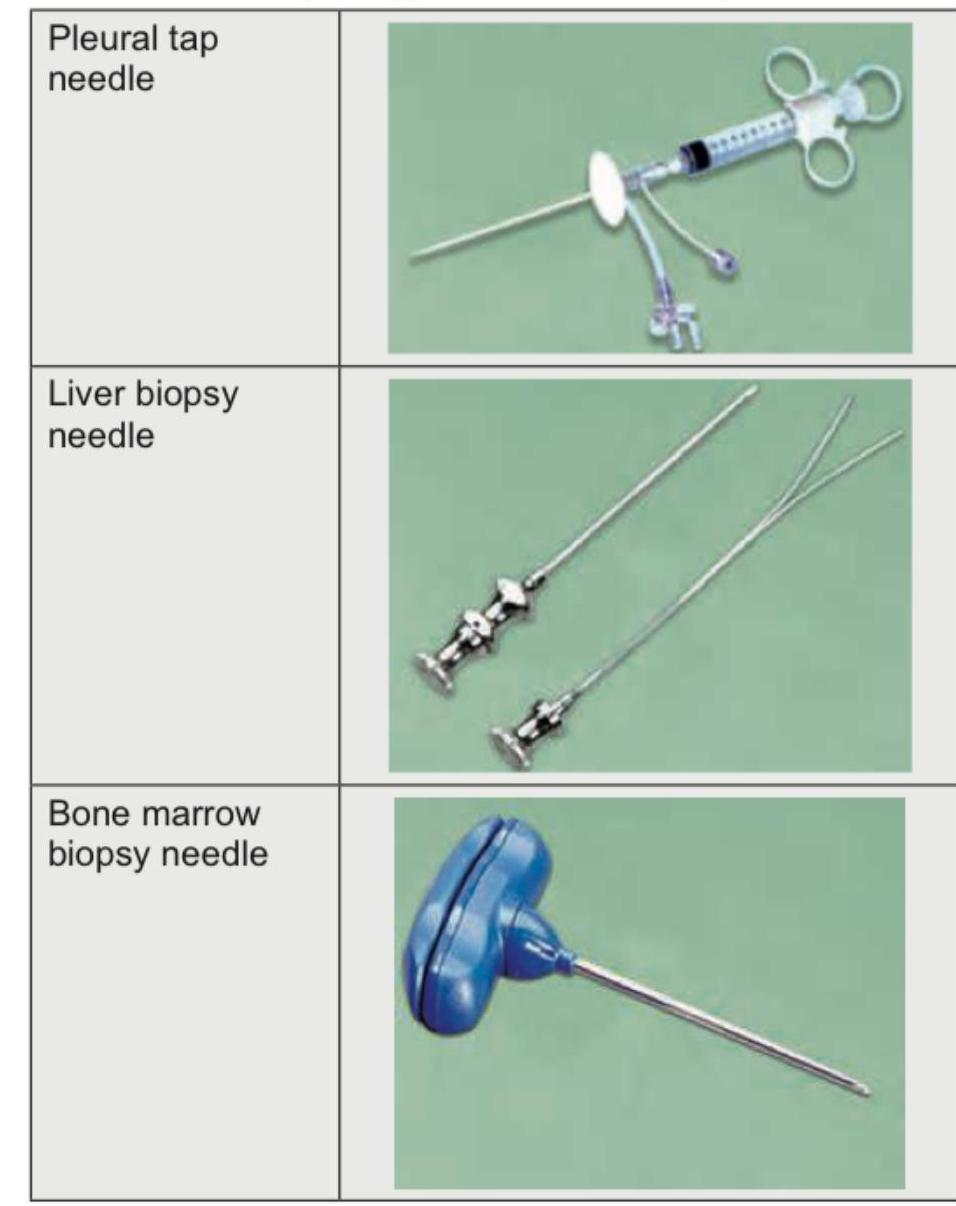
Identify the instrument shown in the figure below.

Which needle is shown below?
Which of the following are the techniques commonly used to close the raw area after excision of a pilonidal sinus in order to avoid a midline wound? I. Limberg procedure II. Y-V plasty III. Z-plasty IV. Karydakis procedure Select the correct answer using the code given below :
Which of the following statements are correct regarding sutures in surgery? I. Barbed sutures have the advantage of eliminating the need for knots. II. Vertical mattress sutures help in eversion of wound edges. III. Aberdeen knot is used for continuous suturing. IV. Silk is preferred for subcuticular suturing. Select the answer using the code given below :
A surgeon is about to start a laparoscopic procedure on a patient. The floor nurse asks the surgeon about the identity of the patient, site of the procedure to be performed and any anticipated critical events during the surgery. These questions are a part of the
Which surgery is most likely to disturb the paracervical nerve plexus resulting in atonicity of the bladder?
Practice by Chapter
Wound Healing and Care
Practice Questions
Surgical Infections
Practice Questions
Fluid and Electrolyte Management
Practice Questions
Nutrition in Surgical Patients
Practice Questions
Hemostasis and Blood Transfusion
Practice Questions
Surgical Instruments and Equipment
Practice Questions
Sutures and Stapling Devices
Practice Questions
Minimal Access Surgery Principles
Practice Questions
Surgical Complications
Practice Questions
Anesthesia Principles for Surgeons
Practice Questions
Surgical Oncology Principles
Practice Questions
Evidence-Based Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app