
General Surgery Principles — MCQs

On this page
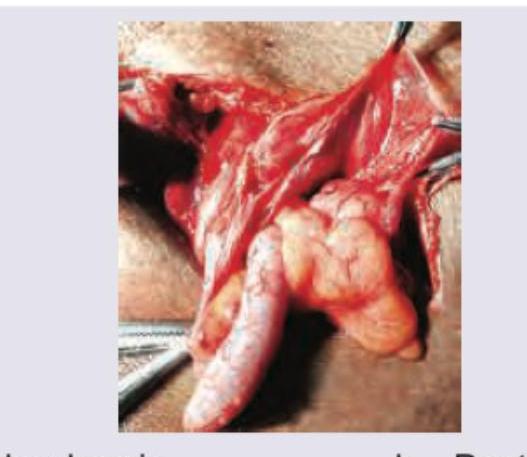
Contents of the inguinal hernia sac are displayed intraoperatively and appendix is seen at 7 o'clock. What is the diagnosis?
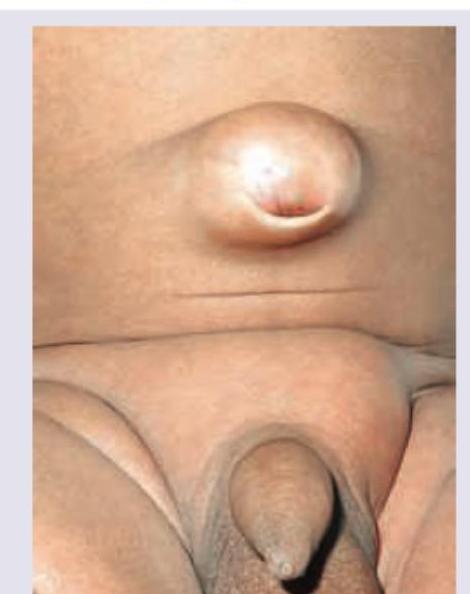
A 35-year-old patient presents with a painless swelling at the umbilicus that has been gradually increasing in size over the past 6 months. The swelling increases on coughing and straining. On examination, there is a reducible bulge at the umbilicus. What is the likely diagnosis?
What is the functional capability of the instrument shown in the image?

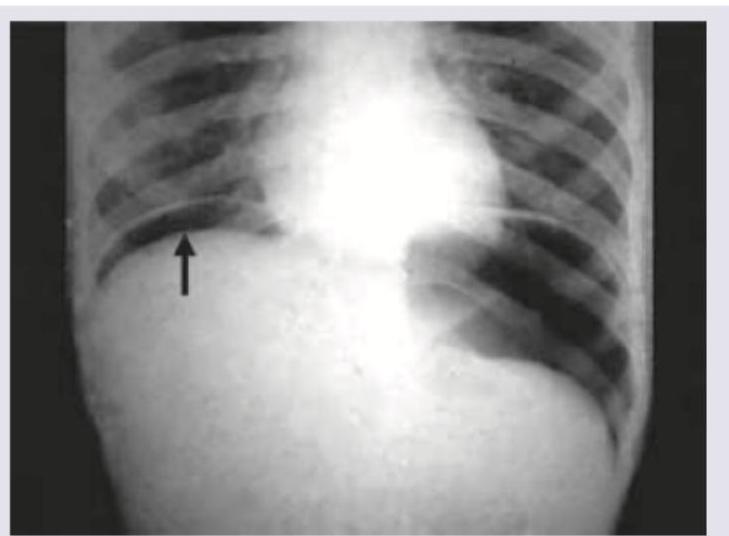
A 30-year-old patient presents with abdominal pain, fever, nausea, vomiting and respiratory distress. On admission BP=80/40 mm Hg and pulse rate is 120 BPM. The following CXR was performed. What is the immediate management? (AIIMS May 2016)
What type of suture is this?
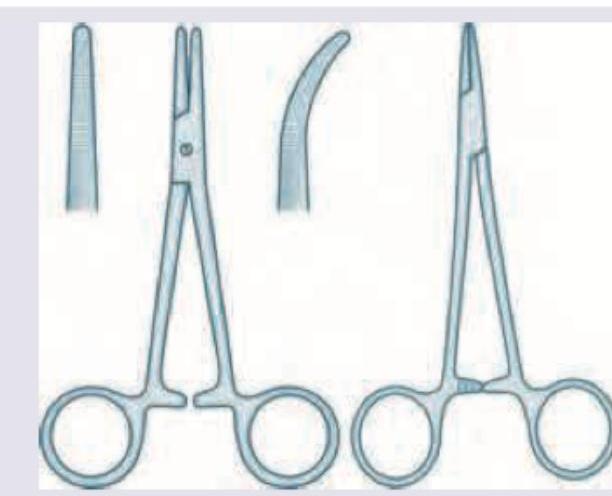
Identify these two surgical instruments.
The following suture material gets absorbed in how many days?

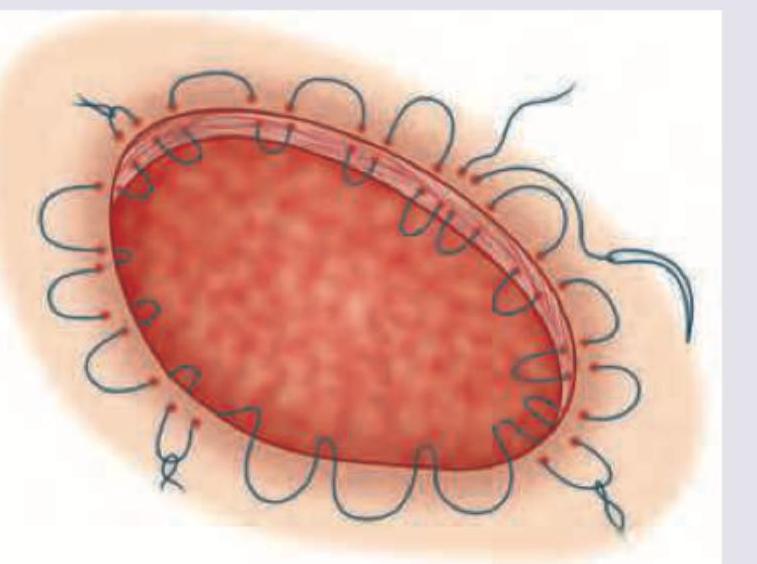
The method of ulcer healing shown below generates a pressure of: (Recent NEET Pattern 2016-17)

Which is correct about the suture material shown in the image?

Which retractor is shown in the image?

Practice by Chapter
Wound Healing and Care
Practice Questions
Surgical Infections
Practice Questions
Fluid and Electrolyte Management
Practice Questions
Nutrition in Surgical Patients
Practice Questions
Hemostasis and Blood Transfusion
Practice Questions
Surgical Instruments and Equipment
Practice Questions
Sutures and Stapling Devices
Practice Questions
Minimal Access Surgery Principles
Practice Questions
Surgical Complications
Practice Questions
Anesthesia Principles for Surgeons
Practice Questions
Surgical Oncology Principles
Practice Questions
Evidence-Based Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app