
General Surgery Principles — MCQs

On this page
Identify the instrument:

Identify the image shown:

The image shows a catheter. What does inscription 18 on the catheter imply?

Which of the following statements regarding the given image is false?

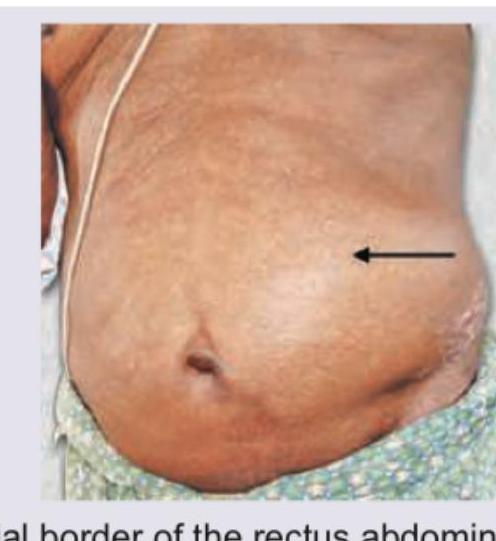
Hernia that is depicted in the image usually occurs at:
All of the following conditions are visible in the image except: (Recent NEET Pattern 2016-17)
A multiparous female presents with the condition shown in the image. This condition can be managed by: (Recent NEET Pattern 2016-17)

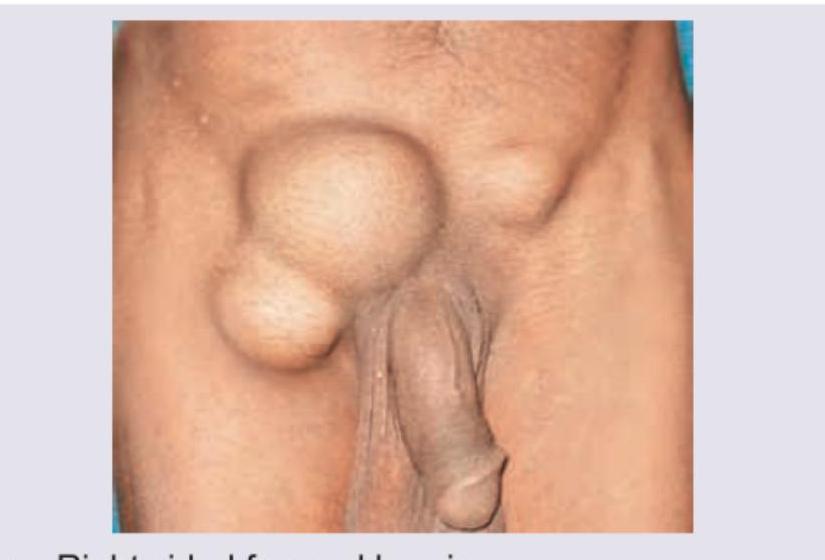
What is the most likely diagnosis based on the clinical image?

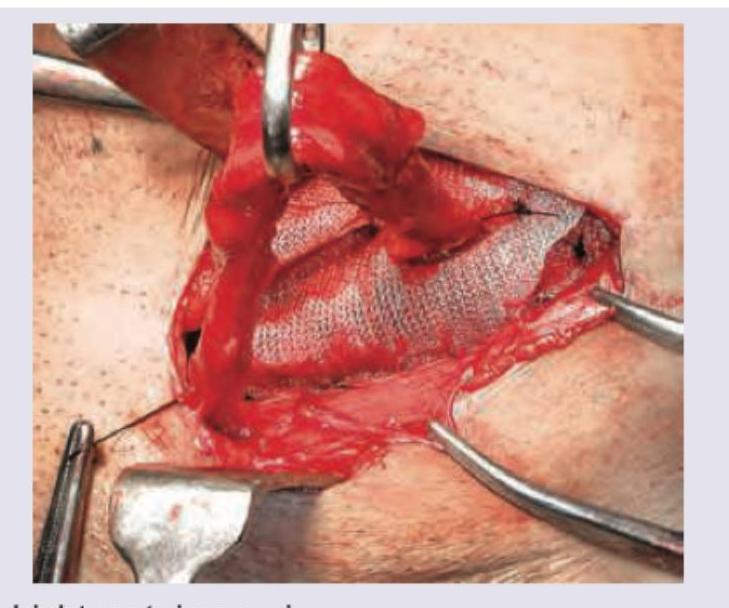
Which hernia repair procedure is shown in the image? (Recent NEET Pattern 2016-17)
A 25-year-old male presents with inguinal swelling. He had surgery for acute abdomen 2 years ago but could not tell the reason behind it. Trauma to which structure during the surgery conducted 2 years ago would have resulted in this inguinal swelling?
Practice by Chapter
Wound Healing and Care
Practice Questions
Surgical Infections
Practice Questions
Fluid and Electrolyte Management
Practice Questions
Nutrition in Surgical Patients
Practice Questions
Hemostasis and Blood Transfusion
Practice Questions
Surgical Instruments and Equipment
Practice Questions
Sutures and Stapling Devices
Practice Questions
Minimal Access Surgery Principles
Practice Questions
Surgical Complications
Practice Questions
Anesthesia Principles for Surgeons
Practice Questions
Surgical Oncology Principles
Practice Questions
Evidence-Based Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app