
General Surgery Principles — MCQs

On this page
The term "universal tumor" refers to which of the following?
What is the most common clinical presentation of basal cell carcinoma?
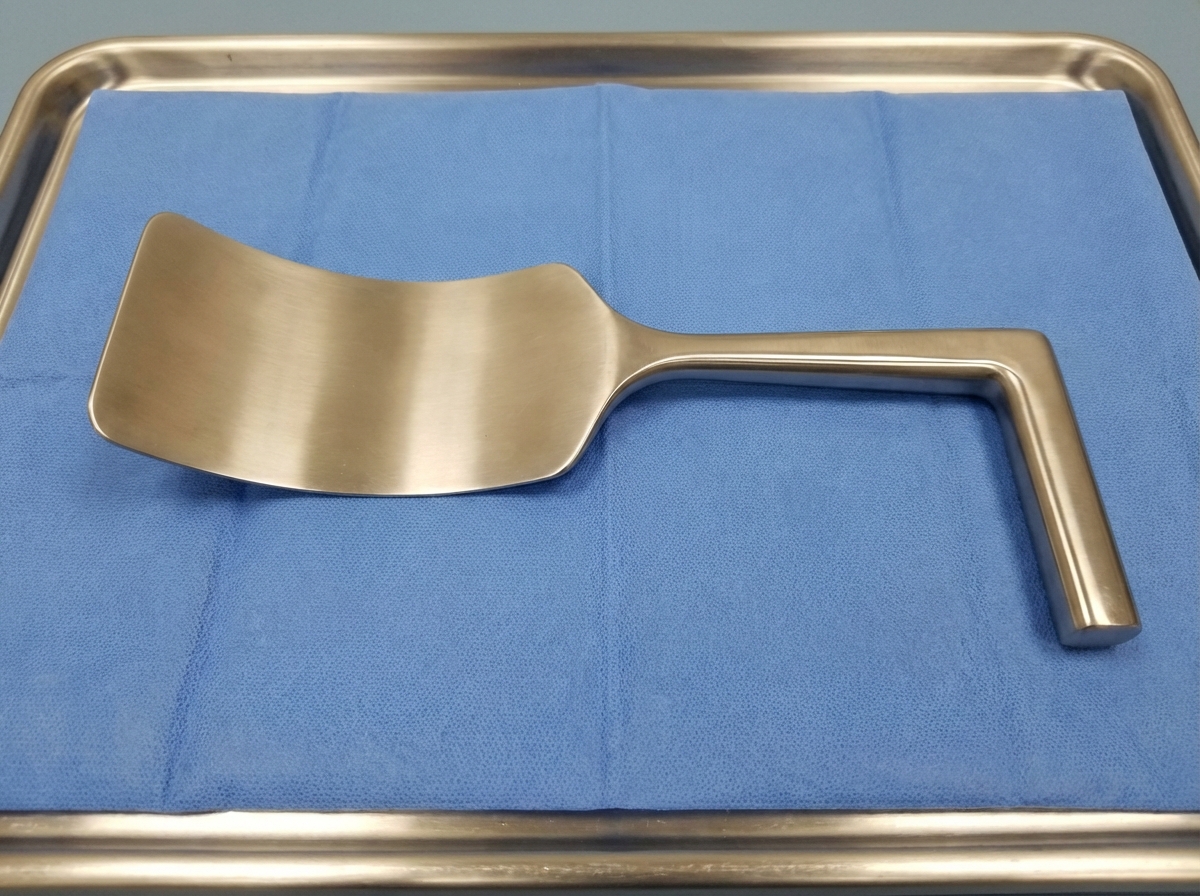
What is the instrument shown below?

Non-blanchable erythema of the skin is classified as which stage of a decubitus ulcer?
Odontoma is treated by:
Which of the following suture materials is absorbable?
Using monopolar cautery during circumcision in children is not advised due to the risk of penile coagulation. What is the mechanism behind this phenomenon?
What is the name of the retractor shown in the image?
What is the most common type of cyst found in the spleen?
Marjolin's ulcer is a:
Practice by Chapter
Wound Healing and Care
Practice Questions
Surgical Infections
Practice Questions
Fluid and Electrolyte Management
Practice Questions
Nutrition in Surgical Patients
Practice Questions
Hemostasis and Blood Transfusion
Practice Questions
Surgical Instruments and Equipment
Practice Questions
Sutures and Stapling Devices
Practice Questions
Minimal Access Surgery Principles
Practice Questions
Surgical Complications
Practice Questions
Anesthesia Principles for Surgeons
Practice Questions
Surgical Oncology Principles
Practice Questions
Evidence-Based Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app