
General Surgery Principles — MCQs

On this page
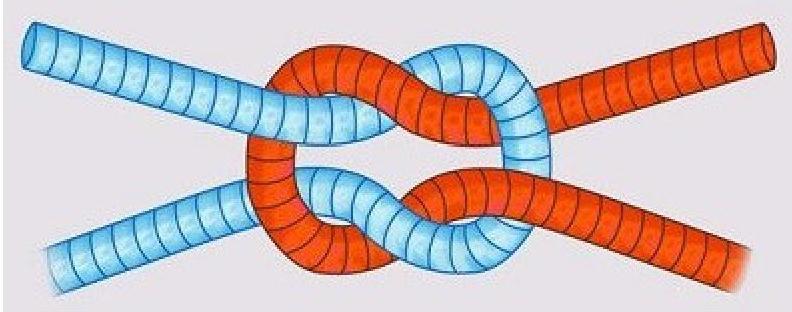
What type of knot is depicted in the image?
Identify the type of retractor shown in the image.

Which of the following statements about keloids is MOST true?
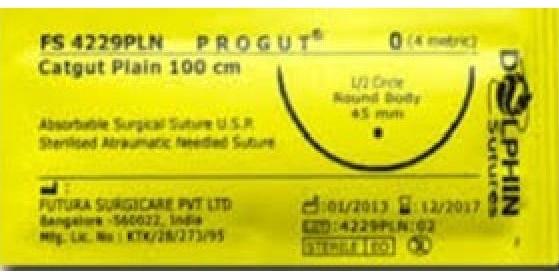
Which of the following statements is true about the suture material shown in the image?
Which type of surgical suture is known to cause the most tissue reaction?
What is the typical absorption duration of Polydioxanone sutures?
Which of the following is NOT a principle of negative pressure wound therapy?
An Incisional wound heals by
Which of the following is the correct management of abdominal compartment syndrome?
Vacuum assisted closure is contraindicated in which of the following conditions -
Practice by Chapter
Wound Healing and Care
Practice Questions
Surgical Infections
Practice Questions
Fluid and Electrolyte Management
Practice Questions
Nutrition in Surgical Patients
Practice Questions
Hemostasis and Blood Transfusion
Practice Questions
Surgical Instruments and Equipment
Practice Questions
Sutures and Stapling Devices
Practice Questions
Minimal Access Surgery Principles
Practice Questions
Surgical Complications
Practice Questions
Anesthesia Principles for Surgeons
Practice Questions
Surgical Oncology Principles
Practice Questions
Evidence-Based Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app