
General Surgery Principles — MCQs

On this page
What is the medical procedure that involves the removal of dead, damaged, or infected tissue from a wound?
Which of the following sutures has maximum tensile strength and minimum tissue reaction?
Most important factor in causation of ingrown toenail is?
For how many weeks do cortisol levels typically remain elevated following a hemorrhage?
Which of the following types of gangrene is least likely to be associated with diabetes?
Which type of healing occurs in an incisional wound with infection?
Which of the following is NOT a criterion for the viability of muscle?
The image below shows a pressure sore. Which stage does this belong to?

Identify the surgical instrument based on the following characteristics: short blades, sharp cutting edges, and a central screw or rivet. Commonly used for cutting sutures.
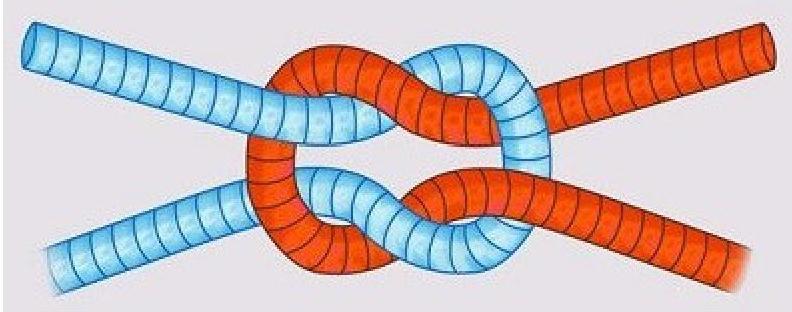
What type of knot is depicted in the image?
Practice by Chapter
Wound Healing and Care
Practice Questions
Surgical Infections
Practice Questions
Fluid and Electrolyte Management
Practice Questions
Nutrition in Surgical Patients
Practice Questions
Hemostasis and Blood Transfusion
Practice Questions
Surgical Instruments and Equipment
Practice Questions
Sutures and Stapling Devices
Practice Questions
Minimal Access Surgery Principles
Practice Questions
Surgical Complications
Practice Questions
Anesthesia Principles for Surgeons
Practice Questions
Surgical Oncology Principles
Practice Questions
Evidence-Based Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app