
General Surgery Principles — MCQs

On this page
Which type of hernia is most likely to result in bowel strangulation?
A 55-year-old male presents with an ulcerative lesion on his leg that does not heal despite treatment. Which condition should be considered?
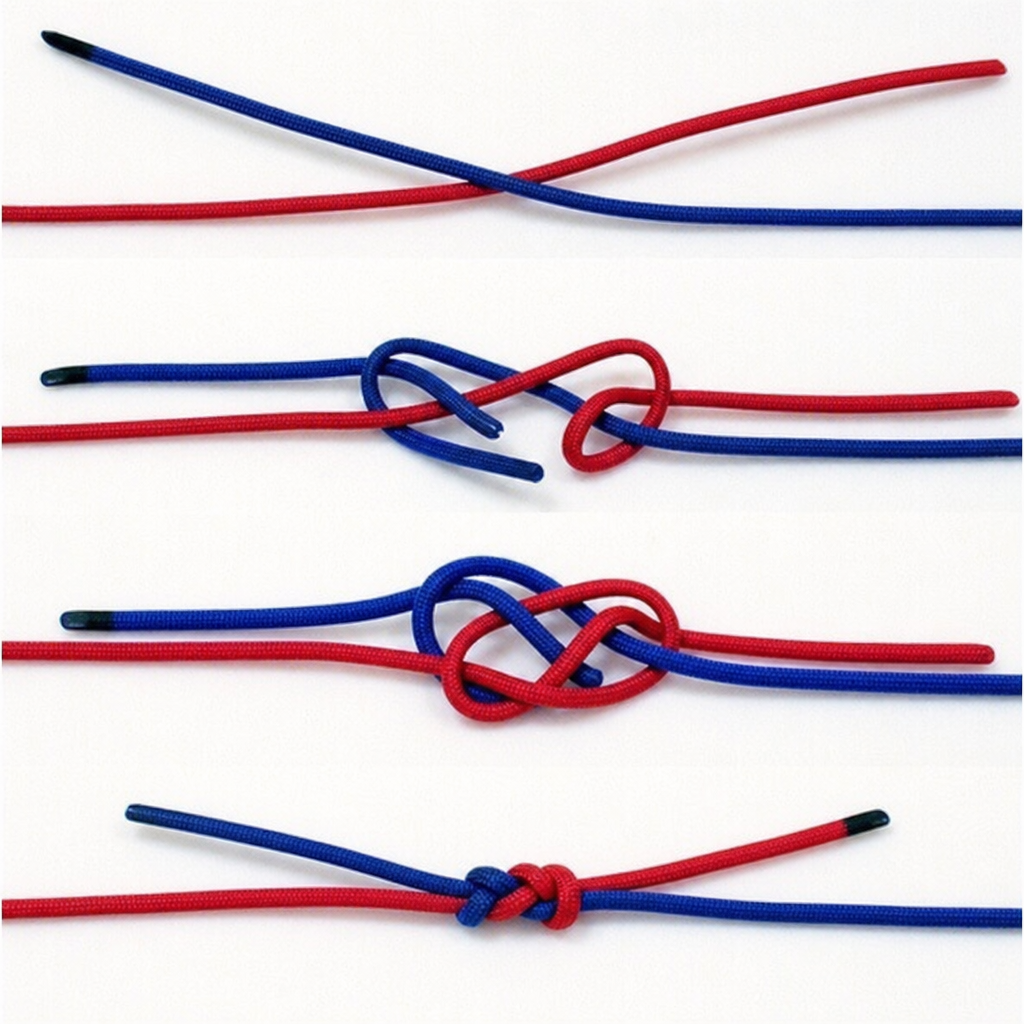
What type of knot is depicted in the image?
Identify the surgical instrument based on its characteristics: a small, triangular blade used for precise incisions.
Which of the following statements is true about absorbable suture materials?
Which type of retractor is shown in the image?

Prolonged surgery time of vaginal hysterectomy may lead to damage to which of the following nerves?
Which of the following is typical of rectus sheath hematoma?
What is the cardinal rule for dressing a pressure ulcer?
Which of the following statements about umbilical hernias is true?
Practice by Chapter
Wound Healing and Care
Practice Questions
Surgical Infections
Practice Questions
Fluid and Electrolyte Management
Practice Questions
Nutrition in Surgical Patients
Practice Questions
Hemostasis and Blood Transfusion
Practice Questions
Surgical Instruments and Equipment
Practice Questions
Sutures and Stapling Devices
Practice Questions
Minimal Access Surgery Principles
Practice Questions
Surgical Complications
Practice Questions
Anesthesia Principles for Surgeons
Practice Questions
Surgical Oncology Principles
Practice Questions
Evidence-Based Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app