
General Surgery Principles — MCQs

On this page
A 65-year-old diabetic woman develops a surgical site infection 5 days after elective cholecystectomy. She has poorly controlled diabetes (HbA1c 10.2%), is obese (BMI 35), and was on chronic steroids for rheumatoid arthritis. Which factor most likely contributed to her delayed wound healing?
A 55-year-old diabetic woman develops necrotizing fasciitis of the perineum following a minor gynecologic procedure. She has septic shock, multiorgan failure, and extensive tissue necrosis. Her family requests 'everything be done,' but her prognosis is poor. Evaluate the ethical and medical approach to her care.
The image shows a Negative Pressure Wound Therapy (NPWT) dressing applied to a patient's wound. What is the standard NPWT pressure setting commonly used to promote wound healing?

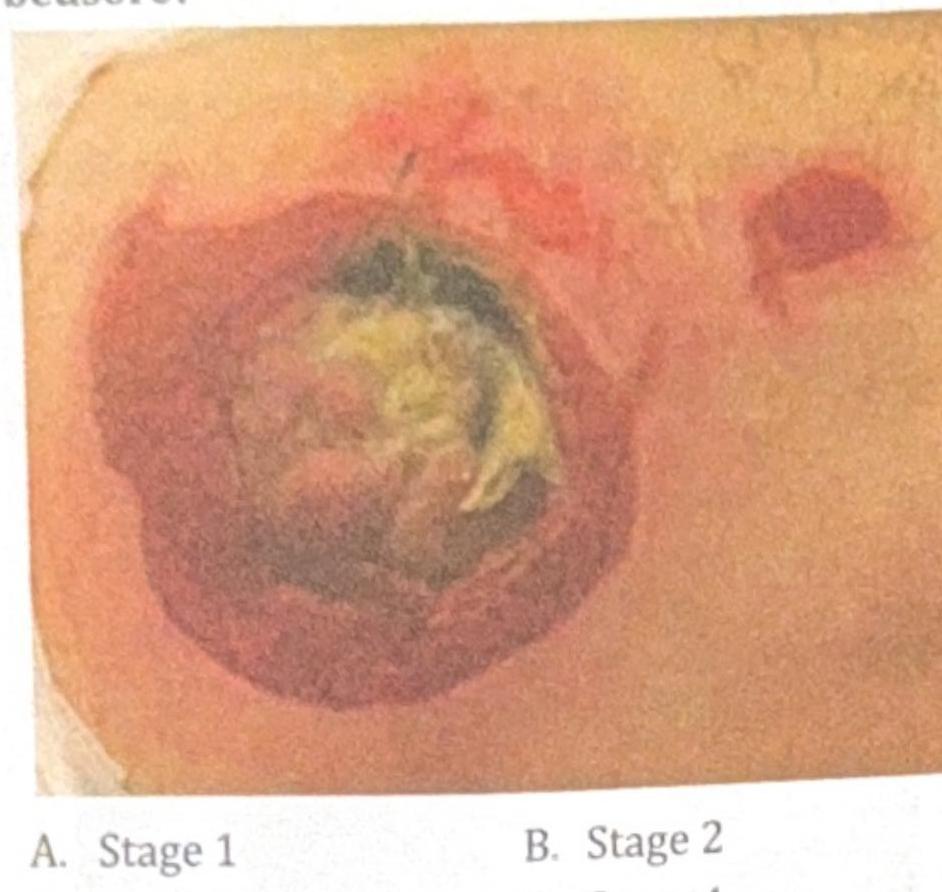
A 78-year-old immobile patient presents with a pressure ulcer on the sacral area, as shown in the image below. How would you grade this bedsore?
Which of the following conditions most commonly presents with free gas under the diaphragm (pneumoperitoneum) on imaging?
A surgeon examined a case of hernia and was able to retract the hernial sac on examination but not the contents. Identify the type of hernia depicted in the image.

You are suturing a laceration in the ER using the interrupted suturing technique. What is the angle of needle placement?
Marjolin's ulcer is:-
Most common immediate complication after splenectomy?
Degloving injury is -
Practice by Chapter
Wound Healing and Care
Practice Questions
Surgical Infections
Practice Questions
Fluid and Electrolyte Management
Practice Questions
Nutrition in Surgical Patients
Practice Questions
Hemostasis and Blood Transfusion
Practice Questions
Surgical Instruments and Equipment
Practice Questions
Sutures and Stapling Devices
Practice Questions
Minimal Access Surgery Principles
Practice Questions
Surgical Complications
Practice Questions
Anesthesia Principles for Surgeons
Practice Questions
Surgical Oncology Principles
Practice Questions
Evidence-Based Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app