
General Surgery Principles — MCQs

On this page
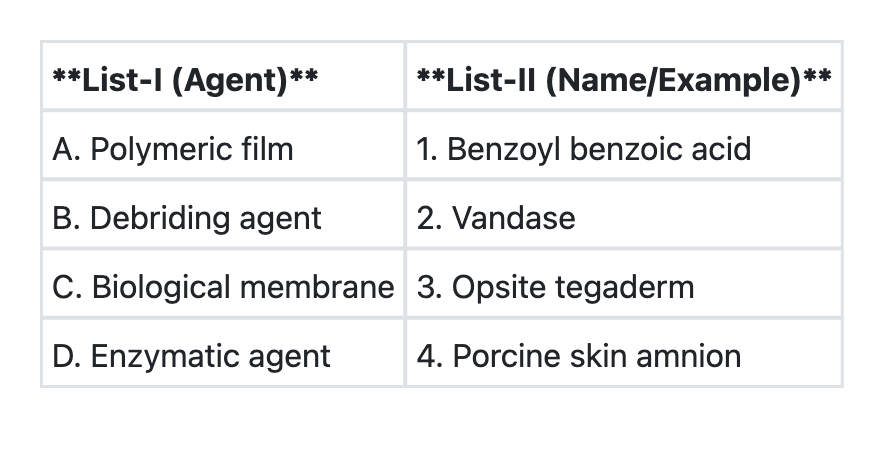
Match List-I with List-II and select the correct answer using the code given below the Lists:
All of the following statements are true for keloids EXCEPT:
All of the following are congenital sinuses except:
The main principle regarding removal of drain after surgery is
A 60 year old lady had a pyothorax which was treated with an intercostal chest drain. After two days, the meniscus of the fluid in the tube was not swinging during her respiratory process. What could be the likely problem?
In Hernia repair, polypropylene suture is used because
Which one of the following regarding absorbable meshes is NOT true?
Untidy wounds are characterised by which of the following? 1. Crushed or avulsed tissues 2. Contaminated wound 3. Devitalised tissue 4. No loss of tissue
Which of the following are types of wound healing? 1. Primary Intention 2. Secondary Intention 3. Tertiary Intention 4. Quaternary Intention
The following are features of hypovolemic shock except:
Practice by Chapter
Wound Healing and Care
Practice Questions
Surgical Infections
Practice Questions
Fluid and Electrolyte Management
Practice Questions
Nutrition in Surgical Patients
Practice Questions
Hemostasis and Blood Transfusion
Practice Questions
Surgical Instruments and Equipment
Practice Questions
Sutures and Stapling Devices
Practice Questions
Minimal Access Surgery Principles
Practice Questions
Surgical Complications
Practice Questions
Anesthesia Principles for Surgeons
Practice Questions
Surgical Oncology Principles
Practice Questions
Evidence-Based Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app