
General Surgery Principles — MCQs

On this page
A surgeon is about to start a laparoscopic procedure on a patient. The floor nurse asks the surgeon about the identity of the patient, site of the procedure to be performed and any anticipated critical events during the surgery. These questions are a part of the
Which of the following are true about epidermal cyst? 1. It is lined by stratified squamous epithelium. 2. It is derived from hair follicle. 3. It contains keratin debris. 4. It is not fixed to the skin.
Which of the following is the PRIMARY factor that predisposes to the development of incisional hernia?
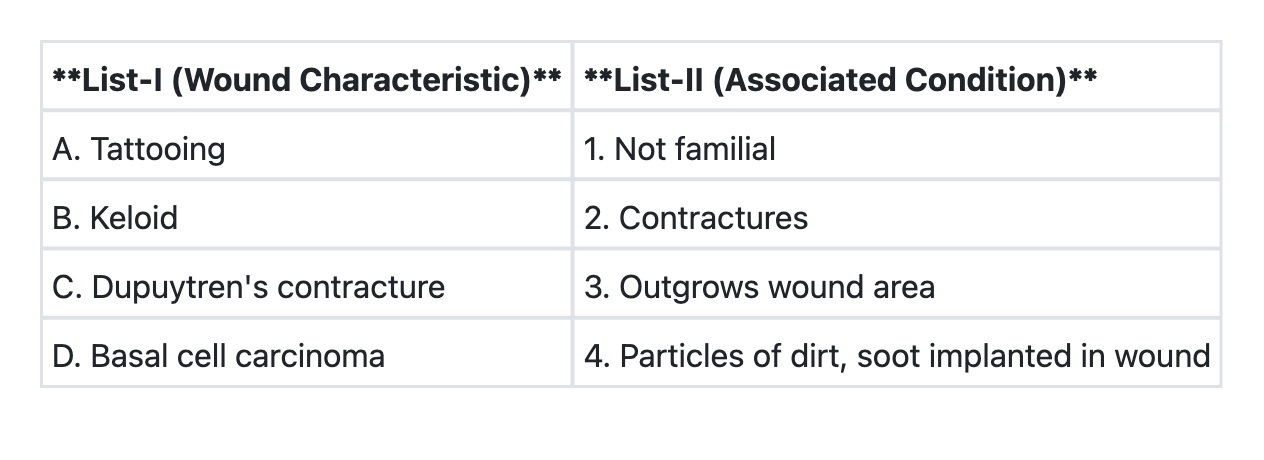
Match List-I with List-II and select the correct answer using the code given below the Lists: (Refer to the image for List-I and List-II)
Consider the following statements regarding splenectomy : 1. It corrects anemia in congenital hereditary spherocytosis. 2. Postponed until the age of 4 years if possible. 3. Polyvalent pneumococcal vaccine to be administered to all before the surgery. Which of the statements given above are correct ?
Splenectomy is best indicated for :
Splenectomy is indicated in all of the following conditions, except
Which of the following statements is true regarding wound contracture ?
The term "debridement of the wound" refers to
Tidy wounds inflicted by sharp instruments and containing no devitalised tissues are expected to heal by
Practice by Chapter
Wound Healing and Care
Practice Questions
Surgical Infections
Practice Questions
Fluid and Electrolyte Management
Practice Questions
Nutrition in Surgical Patients
Practice Questions
Hemostasis and Blood Transfusion
Practice Questions
Surgical Instruments and Equipment
Practice Questions
Sutures and Stapling Devices
Practice Questions
Minimal Access Surgery Principles
Practice Questions
Surgical Complications
Practice Questions
Anesthesia Principles for Surgeons
Practice Questions
Surgical Oncology Principles
Practice Questions
Evidence-Based Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app