
General Surgery Principles — MCQs

On this page
The following image shows:

A 25-year-old man with a history of road traffic injury presents to your clinic 4 months after the episode. His clinical presentation is shown in the image. What is the most likely diagnosis?

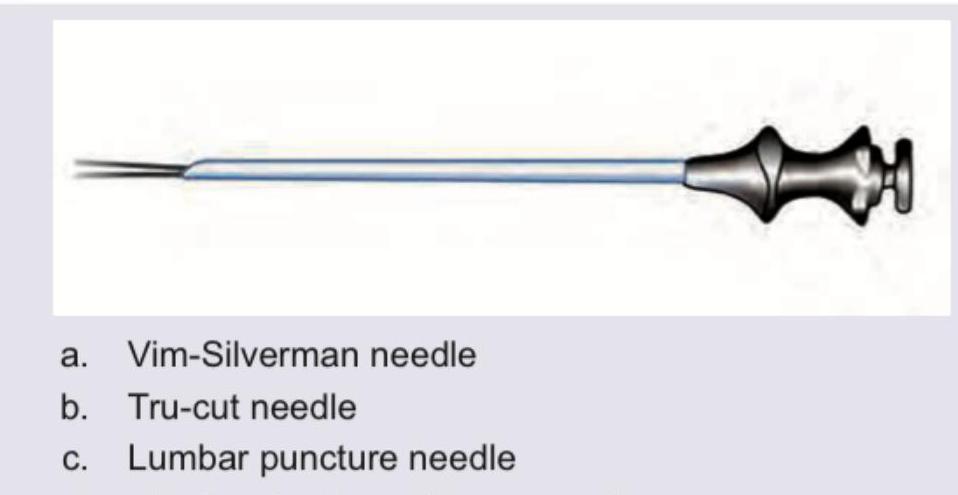
Which needle is shown below?
The commonest site of pressure sore is :
Which of the following are the techniques commonly used to close the raw area after excision of a pilonidal sinus in order to avoid a midline wound? I. Limberg procedure II. Y-V plasty III. Z-plasty IV. Karydakis procedure Select the correct answer using the code given below :
Which of the following statements are correct regarding sutures in surgery? I. Barbed sutures have the advantage of eliminating the need for knots. II. Vertical mattress sutures help in eversion of wound edges. III. Aberdeen knot is used for continuous suturing. IV. Silk is preferred for subcuticular suturing. Select the answer using the code given below :
Consider the following : I. Diabetes II. Hypertension III. Renal failure IV. Jaundice Which of the above are the risk factors for post-operative wound dehiscence?
Which of the following are included in common causes of mediastinal masses in superior and anterior mediastinum? I. Goitre II. Thymic tumour III. Neurogenic tumour Select the correct answer using the code given below :
A 56-year-old male came with acute onset breathlessness and found to have pneumothorax. The resident doctor decided to insert an intercostal drain. Which one of the following sites is suitable for such a procedure?
The best measure of organ perfusion and the best monitor of adequacy of shock therapy is
Practice by Chapter
Wound Healing and Care
Practice Questions
Surgical Infections
Practice Questions
Fluid and Electrolyte Management
Practice Questions
Nutrition in Surgical Patients
Practice Questions
Hemostasis and Blood Transfusion
Practice Questions
Surgical Instruments and Equipment
Practice Questions
Sutures and Stapling Devices
Practice Questions
Minimal Access Surgery Principles
Practice Questions
Surgical Complications
Practice Questions
Anesthesia Principles for Surgeons
Practice Questions
Surgical Oncology Principles
Practice Questions
Evidence-Based Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app