
General Surgery Principles — MCQs

On this page
The following suture material (polyglactin 910) gets absorbed in how many days?

A woman presents 4 days after a laparotomy with complete wound dehiscence. After prescribing antibiotics the surgeon decides to suture the wound. Which of these suture materials should he use?
The method of ulcer healing shown below generates a pressure of: (Recent NEET Pattern 2016-17)

Identify the instrument shown in the image:

Which is correct about the catgut suture material shown in the image?

Which retractor is shown in the image?

A surgical suture material (plain gut) is shown in the image below. Which of the following statements is TRUE about this suture?

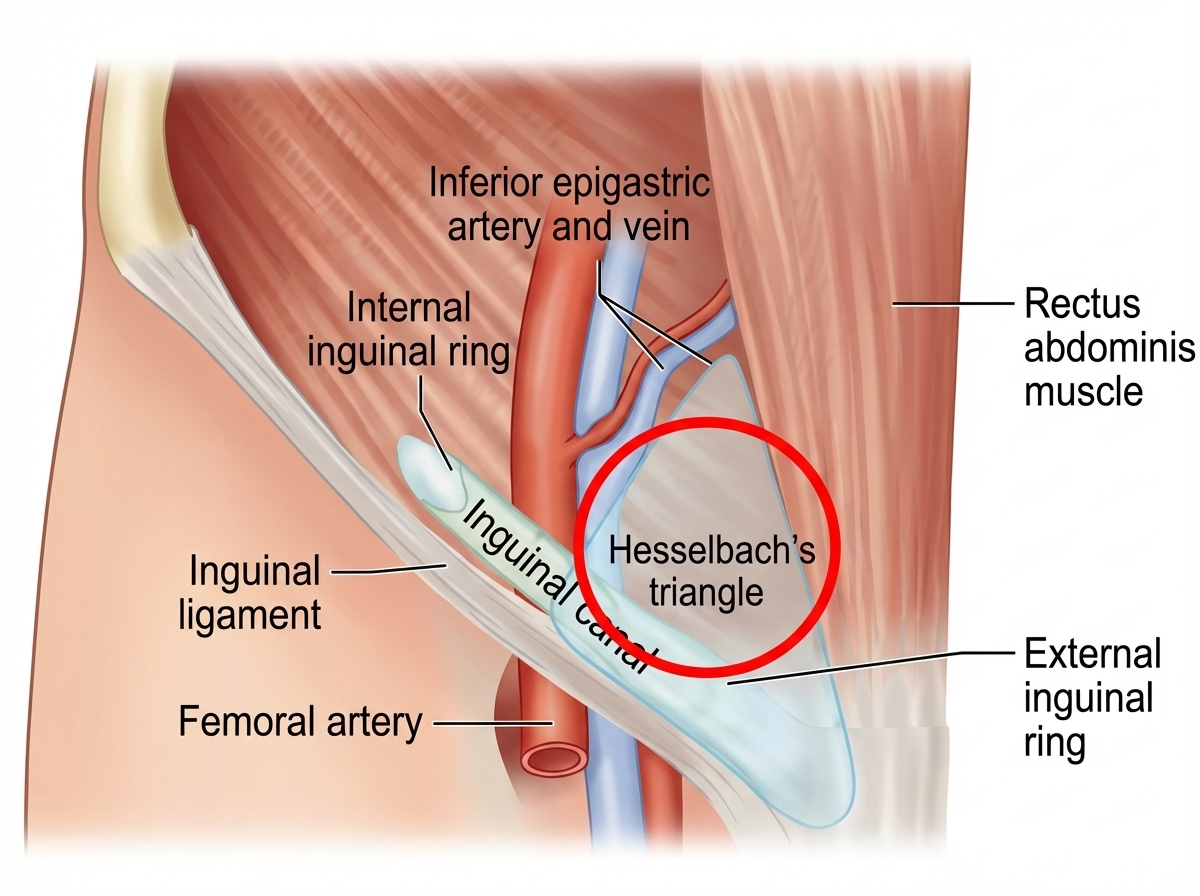
The patient has developed a hernia at the site highlighted by red circle. What is this hernia called as per NYHUS classification? (NEET Pattern 2018)
The image shows a child with acute lymphoblastic leukemia. Identify the type of catheter shown:

A 60-year-old male presents to the emergency department on the second day of symptom onset with progressive deterioration of consciousness due to large right MCA territory infarct. Which of the following is the most appropriate management? (Image: img-179.jpeg)
Practice by Chapter
Wound Healing and Care
Practice Questions
Surgical Infections
Practice Questions
Fluid and Electrolyte Management
Practice Questions
Nutrition in Surgical Patients
Practice Questions
Hemostasis and Blood Transfusion
Practice Questions
Surgical Instruments and Equipment
Practice Questions
Sutures and Stapling Devices
Practice Questions
Minimal Access Surgery Principles
Practice Questions
Surgical Complications
Practice Questions
Anesthesia Principles for Surgeons
Practice Questions
Surgical Oncology Principles
Practice Questions
Evidence-Based Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app