
General Surgery Principles — MCQs

On this page
A 60-year-old male came with bleeding per rectum and was diagnosed to have carcinoma colon. The patient underwent extended hemicolectomy. Identify the instrument the surgeon is using: (AIIMS Nov 2016)

What is the most likely diagnosis based on the image provided? The patient had a snake bite at this site 5 years ago, which left a chronic non-healing ulcer/scar that has now developed into the lesion shown.

A 60-year-old male patient with a history of weight gain and polyuria presents with the following lesion. What is the most possible diagnosis?

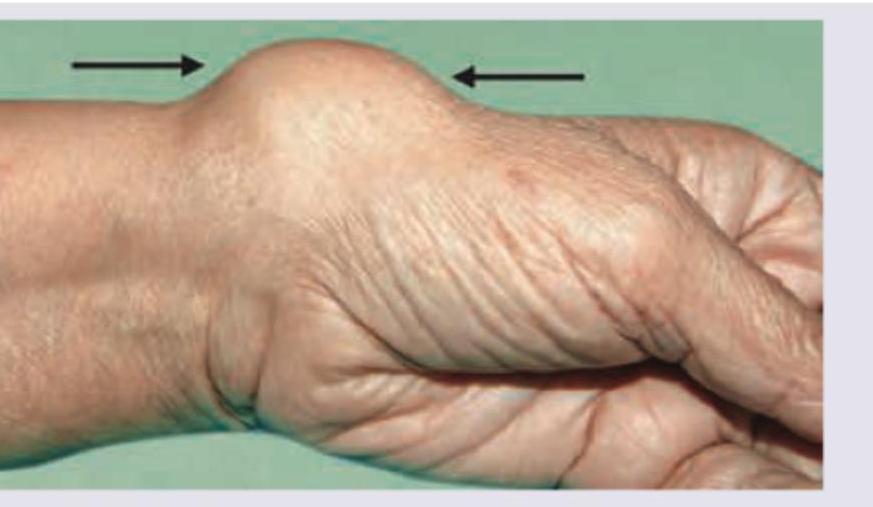
A patient presents with a mass on the volar-radial aspect of the wrist. On examination, the mass is soft, mobile, and nonpulsatile. Ultrasound with Doppler shows a nonvascular subcutaneous fatty lesion. What is the most likely diagnosis?
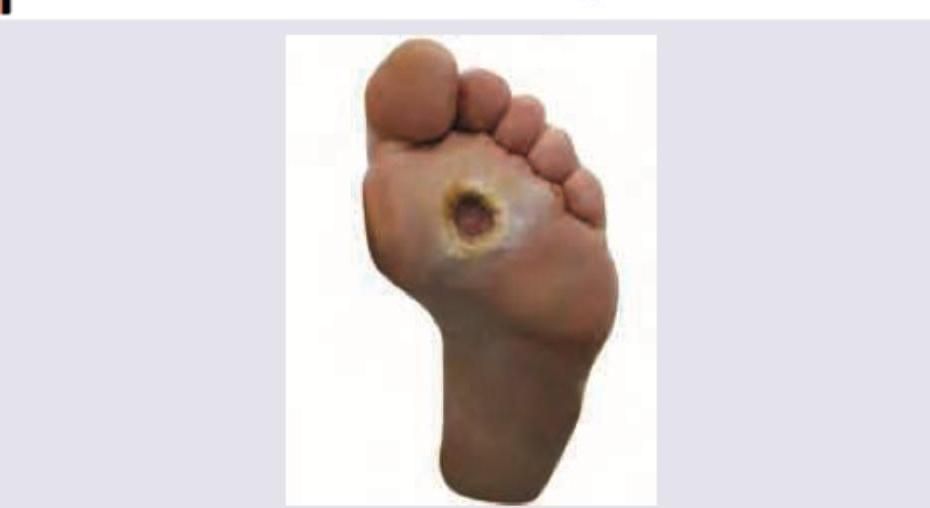
A diabetic patient presents with a plantar foot ulcer. On examination, the ulcer is located beneath the second and third metatarsal heads, has a punched-out appearance with a surrounding callus, shows no signs of active infection, has minimal exudate, and probing does not reach bone. There is no fever, no erythema extending beyond the wound margin, and initial plain radiographs show no bony changes. All are correct about the image shown below except:
All are true about the lesion shown below except:

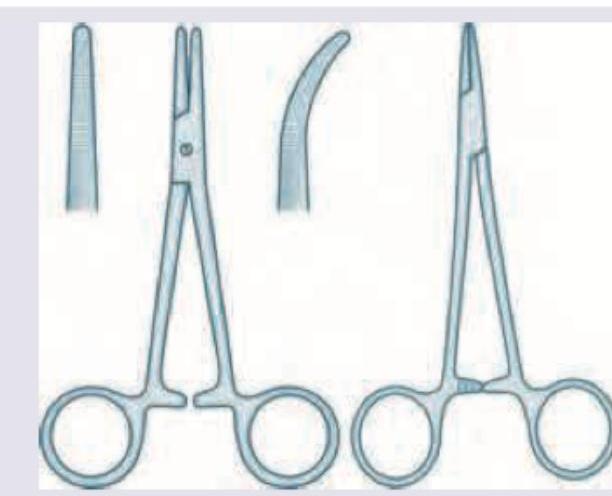
Identify these two surgical instruments.

All are true about the lesion shown below except:

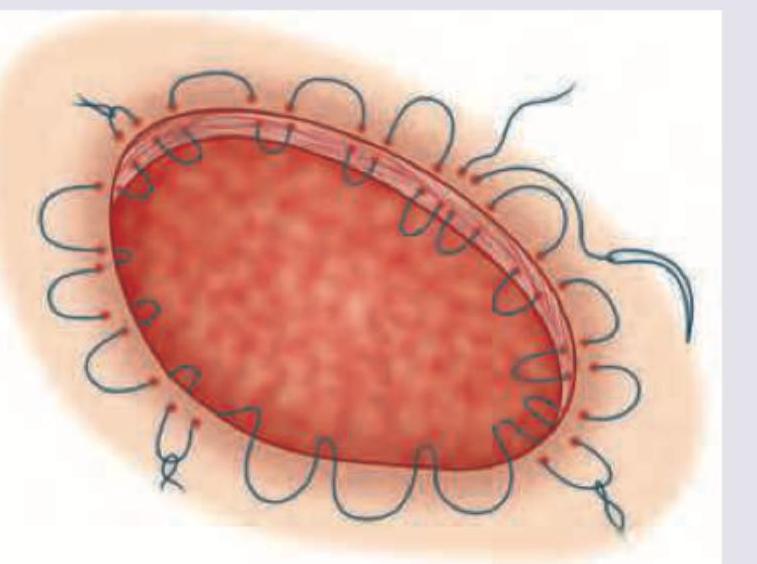
What type of suture is this?
Identify these two surgical instruments.
Practice by Chapter
Wound Healing and Care
Practice Questions
Surgical Infections
Practice Questions
Fluid and Electrolyte Management
Practice Questions
Nutrition in Surgical Patients
Practice Questions
Hemostasis and Blood Transfusion
Practice Questions
Surgical Instruments and Equipment
Practice Questions
Sutures and Stapling Devices
Practice Questions
Minimal Access Surgery Principles
Practice Questions
Surgical Complications
Practice Questions
Anesthesia Principles for Surgeons
Practice Questions
Surgical Oncology Principles
Practice Questions
Evidence-Based Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app