
General Surgery Principles — MCQs

On this page
Identify the instrument in the image:
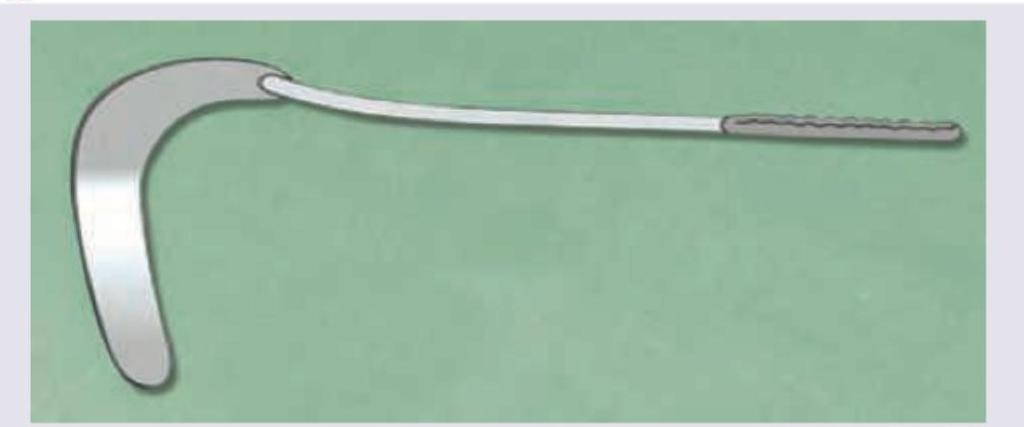
Identify the instrument in the image:

Identify the instrument in the image:

Identify the instrument:

Identify the instrument:

What is the most specific name of this instrument?

Identify the tube/catheter shown in the figure:
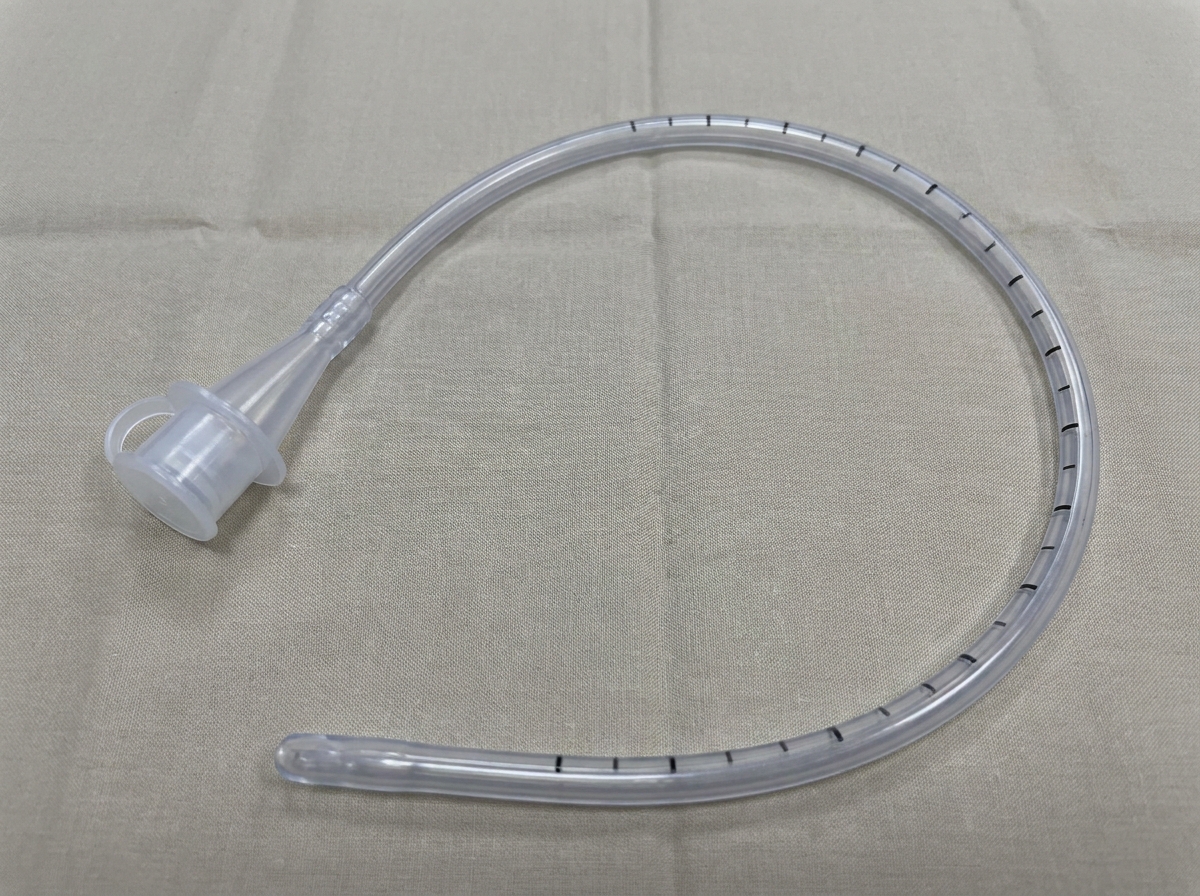
The image shows a catheter. What does inscription 18 on the catheter imply?

A 62-year-old woman presents with a firm, non-tender nodule at the umbilicus. Biopsy confirms metastatic adenocarcinoma. The image shows the clinical appearance of this finding. Which of the following carcinomas is least commonly associated with the condition shown in the image?

What is the functional capability of the instrument shown in the image?

Practice by Chapter
Wound Healing and Care
Practice Questions
Surgical Infections
Practice Questions
Fluid and Electrolyte Management
Practice Questions
Nutrition in Surgical Patients
Practice Questions
Hemostasis and Blood Transfusion
Practice Questions
Surgical Instruments and Equipment
Practice Questions
Sutures and Stapling Devices
Practice Questions
Minimal Access Surgery Principles
Practice Questions
Surgical Complications
Practice Questions
Anesthesia Principles for Surgeons
Practice Questions
Surgical Oncology Principles
Practice Questions
Evidence-Based Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app