
General Surgery Principles — MCQs

On this page
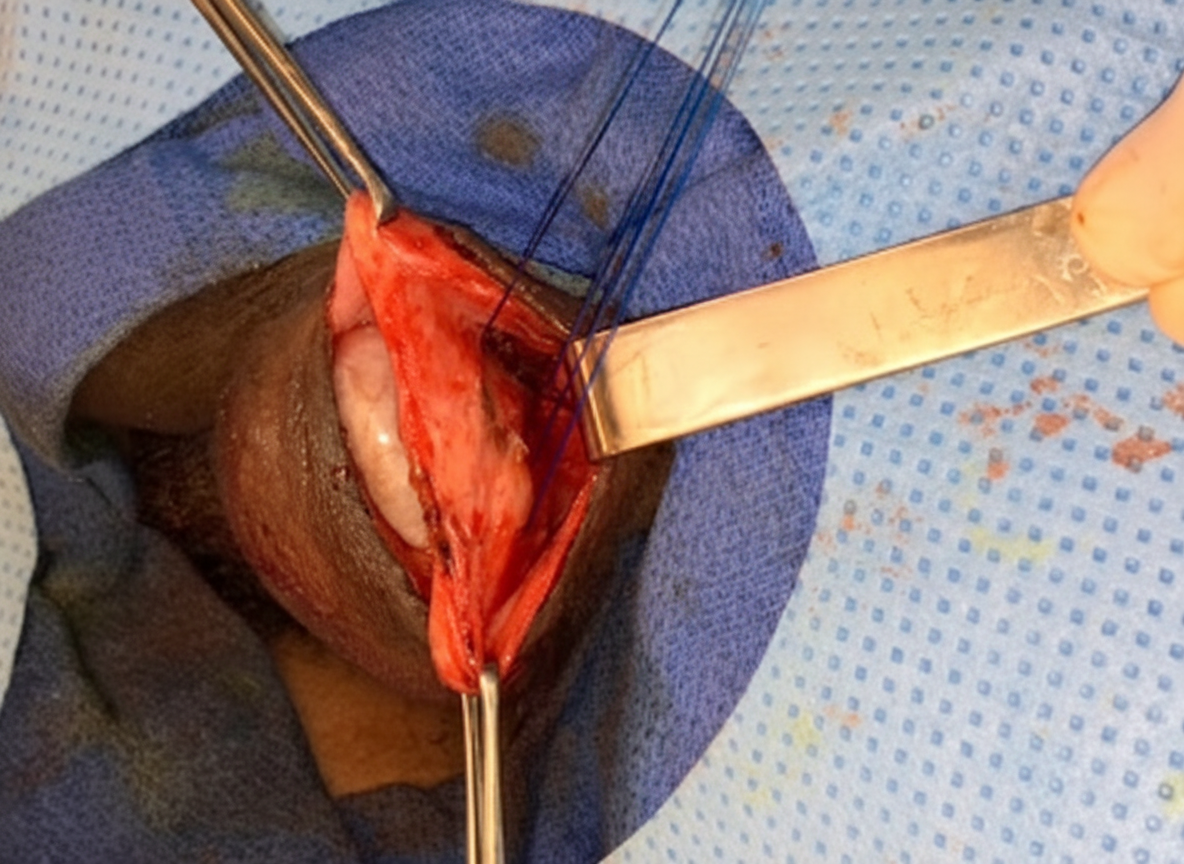
A 25-year-old patient presents to the surgical OPD with a painless left inguinal reducible mass. On examination cough impulse is positive. After further investigations, the patient is diagnosed with an inguinal hernia. What is the surgical management of this patient?
Identify the given instrument.
Elective splenectomy is preferred in which of the following conditions?
Which of the following statements regarding Vacuum-Assisted Closure (VAC) therapy is correct? 1. It promotes granulation tissue formation 2. It reduces interstitial and periwound edema 3. It drains excessive exudate 4. It increases local blood flow
Identify the knot?
What is correct regarding the physical construction of this Prolene (Polypropylene) suture?
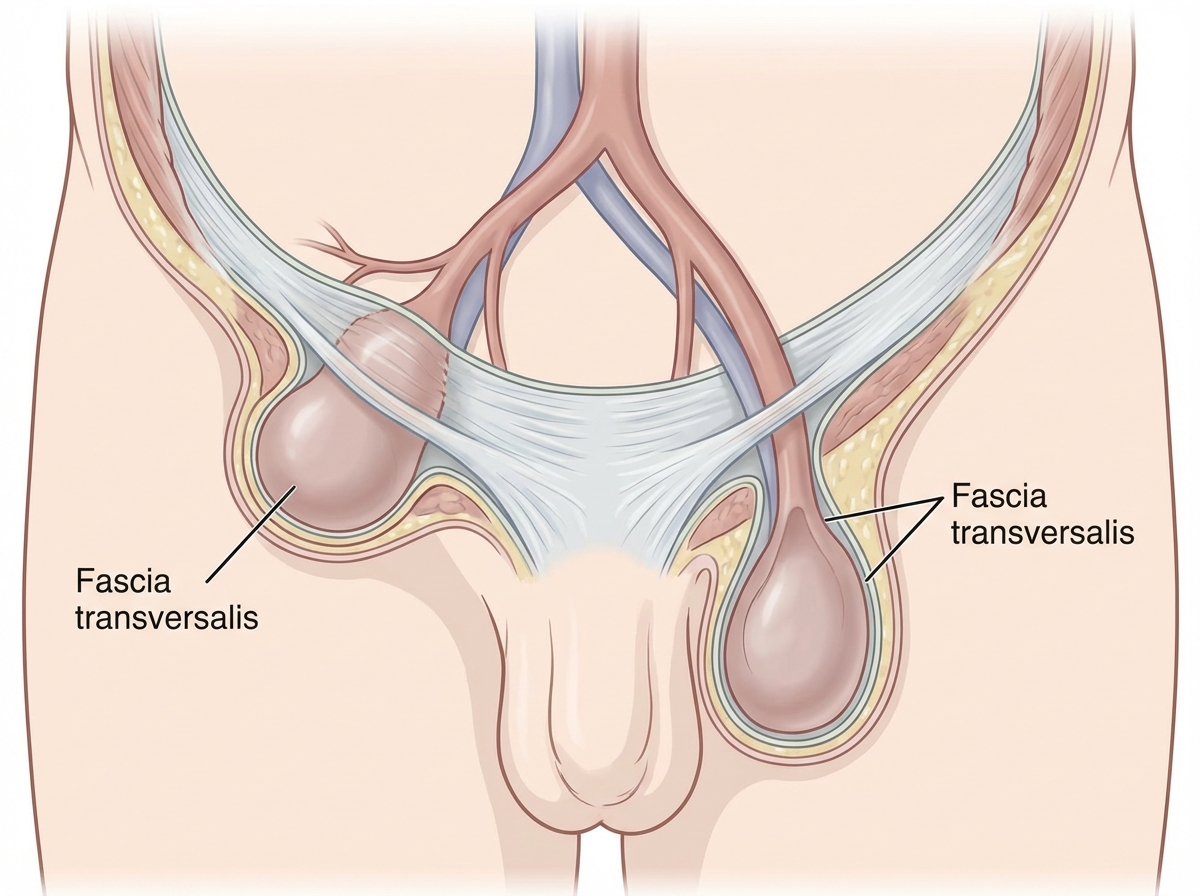
A patient underwent surgery for a reducible groin swelling. The anatomical illustration shows the coverings of the hernia sac, with an arrow marking the identified hernia. Using the reference table below that enumerates the covering layers of inguinal hernias, identify the type of hernia shown: | Indirect inguinal hernia | Direct inguinal hernia | | :--: | :--: | | - Extraperitoneal tissue <br> - Internal spermatic <br> fascia <br> - Cremasteric fascia <br> - External spermatic <br> fascia <br> - Skin | - Extraperitoneal tissue <br> - Fascia transversalis <br> - Conjoint tendon (in medial <br> direct hernia) <br> - Cremaster fascia (in <br> lateral direct hernia) <br> - External spermatic fascia <br> - Skin |
The catgut suture material shown below is sterilized by which method?

What does the given image show?
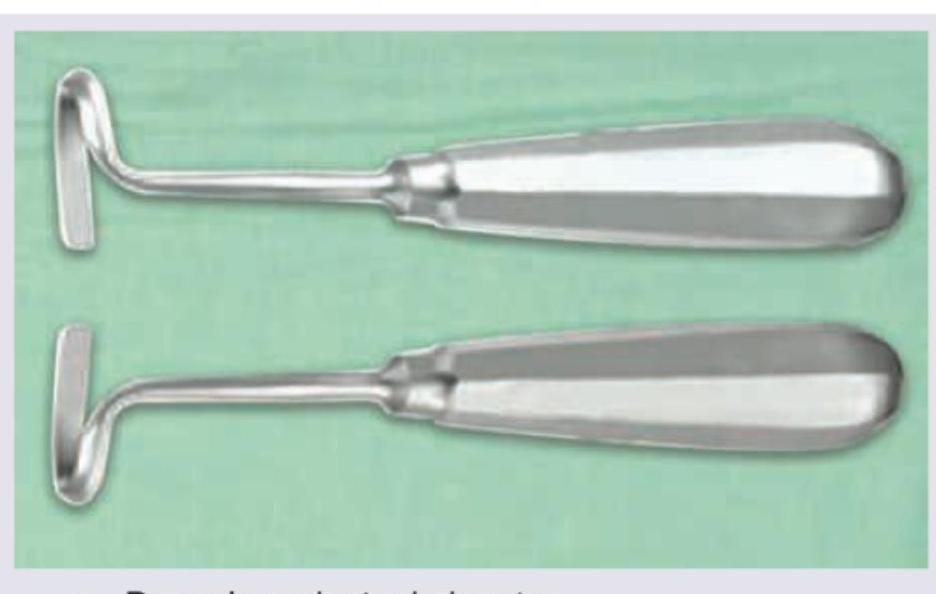
Identify the instrument:

Practice by Chapter
Wound Healing and Care
Practice Questions
Surgical Infections
Practice Questions
Fluid and Electrolyte Management
Practice Questions
Nutrition in Surgical Patients
Practice Questions
Hemostasis and Blood Transfusion
Practice Questions
Surgical Instruments and Equipment
Practice Questions
Sutures and Stapling Devices
Practice Questions
Minimal Access Surgery Principles
Practice Questions
Surgical Complications
Practice Questions
Anesthesia Principles for Surgeons
Practice Questions
Surgical Oncology Principles
Practice Questions
Evidence-Based Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app