
General Surgery Principles — MCQs

On this page
From which of the following sites should a biopsy NOT be taken?
Lung volume reduction surgery is used in the management of which of the following conditions?
Which of the following procedures is associated with the worst prognosis?
What is the major disadvantage of a peripheral intravenous line?
Maximum tissue reaction is associated with which suture material?
A skin ulcer with undermined edges suggests which of the following conditions?
A patient with an abdominal wall desmoid tumor should be screened for which of the following conditions?
What is the most common type of hernia in females?
Colopotomy is done to treat which of the following?
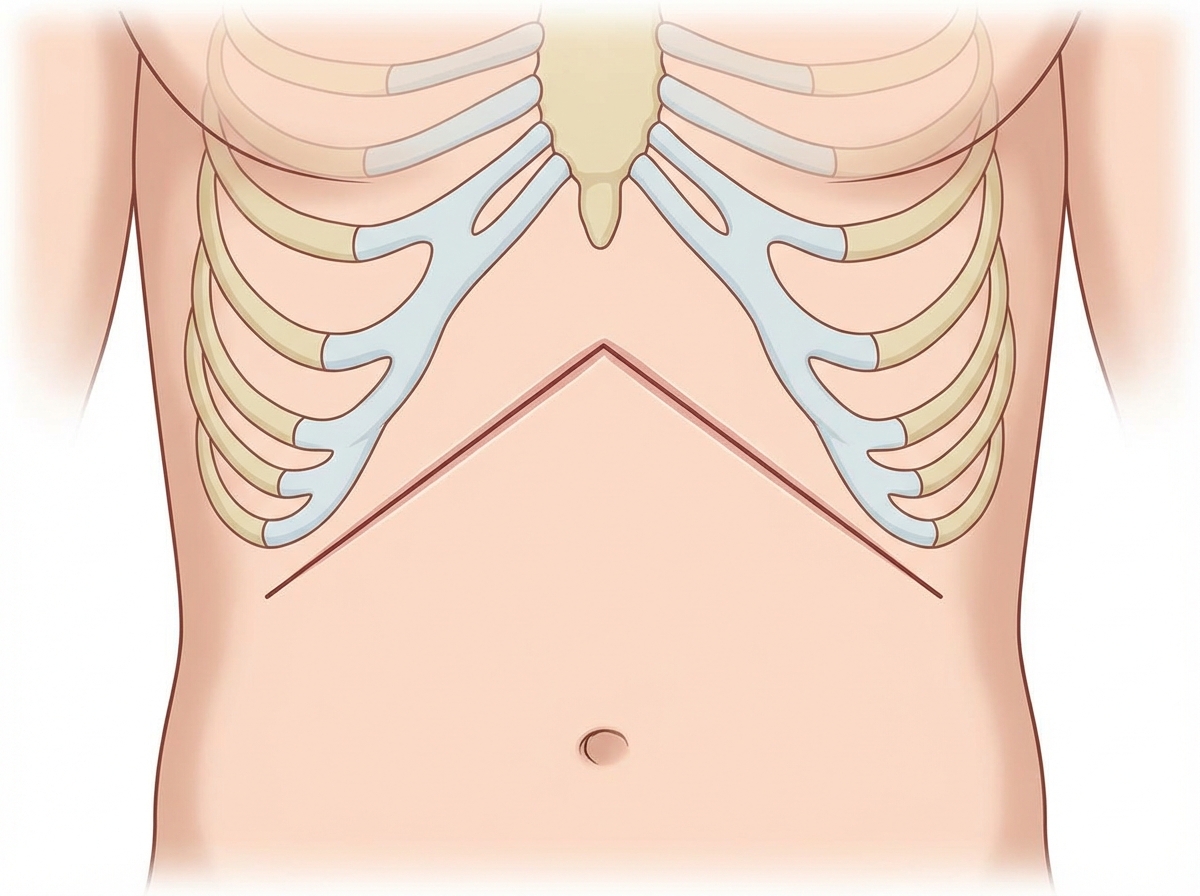
Name the incision.
Practice by Chapter
Wound Healing and Care
Practice Questions
Surgical Infections
Practice Questions
Fluid and Electrolyte Management
Practice Questions
Nutrition in Surgical Patients
Practice Questions
Hemostasis and Blood Transfusion
Practice Questions
Surgical Instruments and Equipment
Practice Questions
Sutures and Stapling Devices
Practice Questions
Minimal Access Surgery Principles
Practice Questions
Surgical Complications
Practice Questions
Anesthesia Principles for Surgeons
Practice Questions
Surgical Oncology Principles
Practice Questions
Evidence-Based Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app