
General Surgery Principles — MCQs

On this page
Massive blood transfusion is defined as?
Which physical principle does this scalpel operate on?

Which of the following is NOT a natural response to injury?
What are the differentiating features between sepsis and trauma?
What is the most common organism causing peritonitis?
In infection involving the submandibular space when extraoral incision and drainage are necessary, which of the following structures must be divided?
Which of the following is NOT an indication for splenectomy?
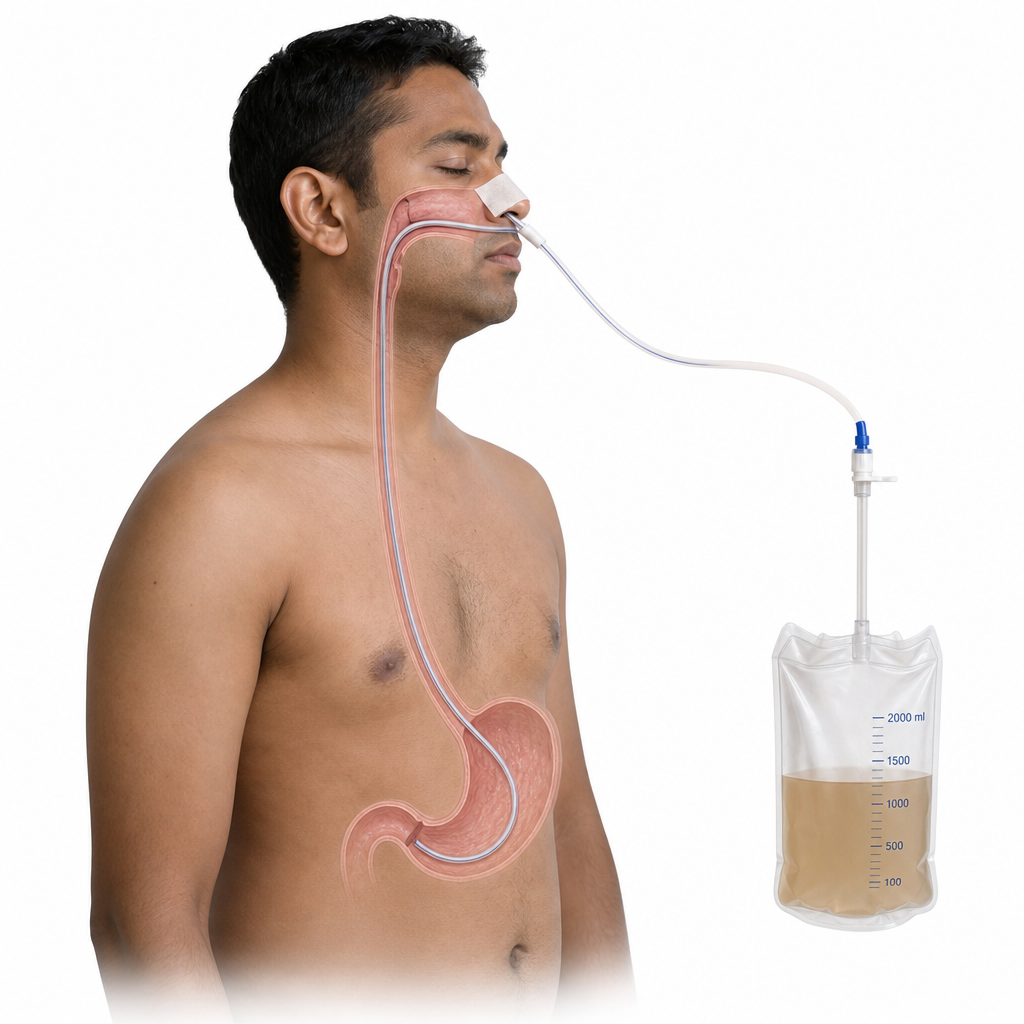
Which of the following is the primary use of the nasogastric tube depicted?
Suturing in facial wound injuries should ideally be performed within what timeframe?
True about indirect inguinal hernia?
Practice by Chapter
Wound Healing and Care
Practice Questions
Surgical Infections
Practice Questions
Fluid and Electrolyte Management
Practice Questions
Nutrition in Surgical Patients
Practice Questions
Hemostasis and Blood Transfusion
Practice Questions
Surgical Instruments and Equipment
Practice Questions
Sutures and Stapling Devices
Practice Questions
Minimal Access Surgery Principles
Practice Questions
Surgical Complications
Practice Questions
Anesthesia Principles for Surgeons
Practice Questions
Surgical Oncology Principles
Practice Questions
Evidence-Based Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app