
Gastrointestinal Surgery — MCQs

On this page
After splenectomy, the most common infection is:
What is the most common cause of intestinal obstruction?
A 45-year-old gentleman has undergone truncal vagotomy and pyloroplasty for bleeding duodenal ulcer seven years ago. Now he has intractable recurrent symptoms of peptic ulcer. All of the following suggest the diagnosis of Zollinger-Ellison syndrome, except:
All are causes of mechanical intestinal obstruction except which of the following?
Which of the following is the MOST significant risk factor for inguinal hernia?
Which type of hernia is commonly associated with hydrocele?
Which of the following statements regarding indirect inguinal hernia is incorrect?
What are the potential symptoms of malignant transformation in a retroperitoneal lipoma?
The most common complication of Zenker's diverticulum is:
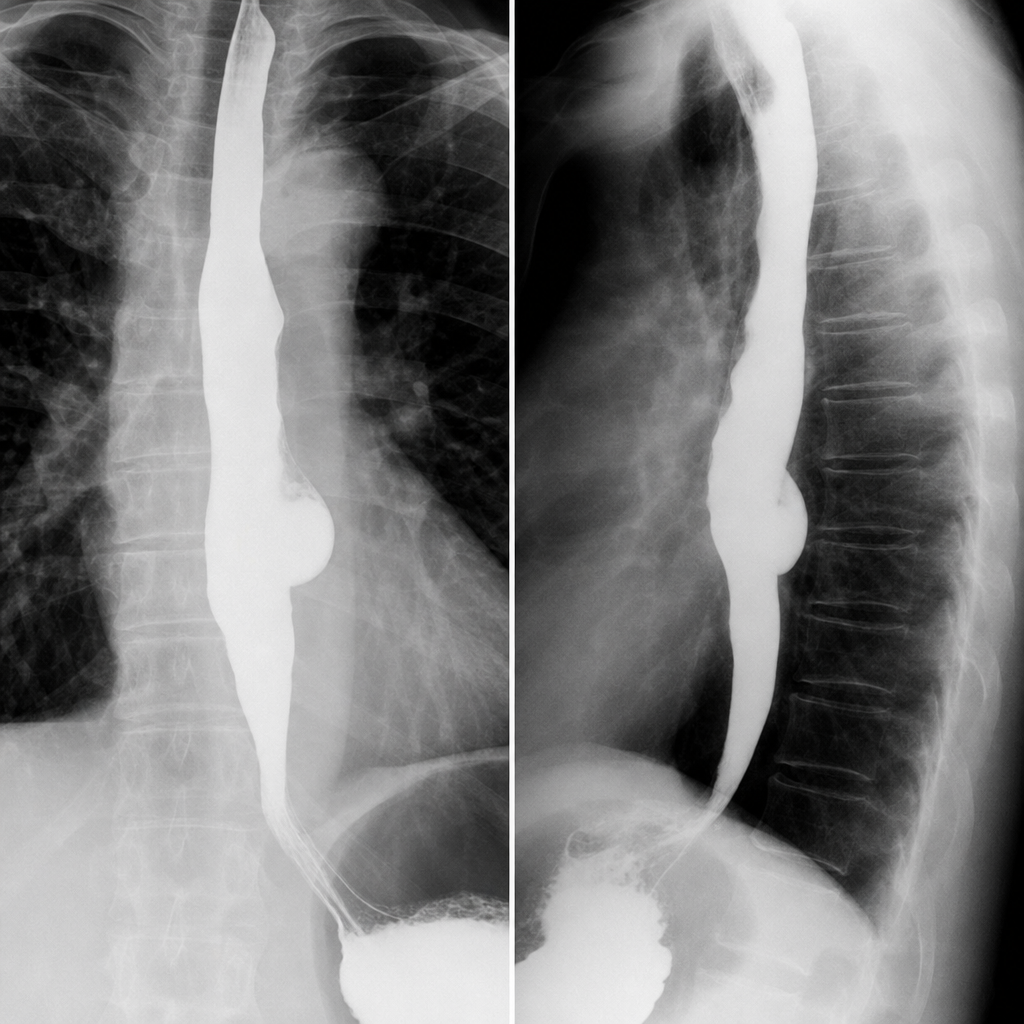
A 69-year-old man is informed that the cause of his dysphagia is a benign lesion. The barium swallow is shown in the figure below. What should he be told regarding benign tumors and cysts of the esophagus?
Practice by Chapter
Esophageal Disorders
Practice Questions
Gastric Disorders
Practice Questions
Small Intestine Pathology
Practice Questions
Appendicitis
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Intestinal Obstruction
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Diverticular Disease
Practice Questions
Anorectal Disorders
Practice Questions
Colorectal Neoplasms
Practice Questions
Gastrointestinal Stomas
Practice Questions
Bariatric Surgery Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app