
Gastrointestinal Surgery — MCQs

On this page
What is the investigation of choice for esophageal rupture?
What is the best treatment for esophageal carcinoma in situ?
Which of the following is not a risk factor for carcinoma of the esophagus?
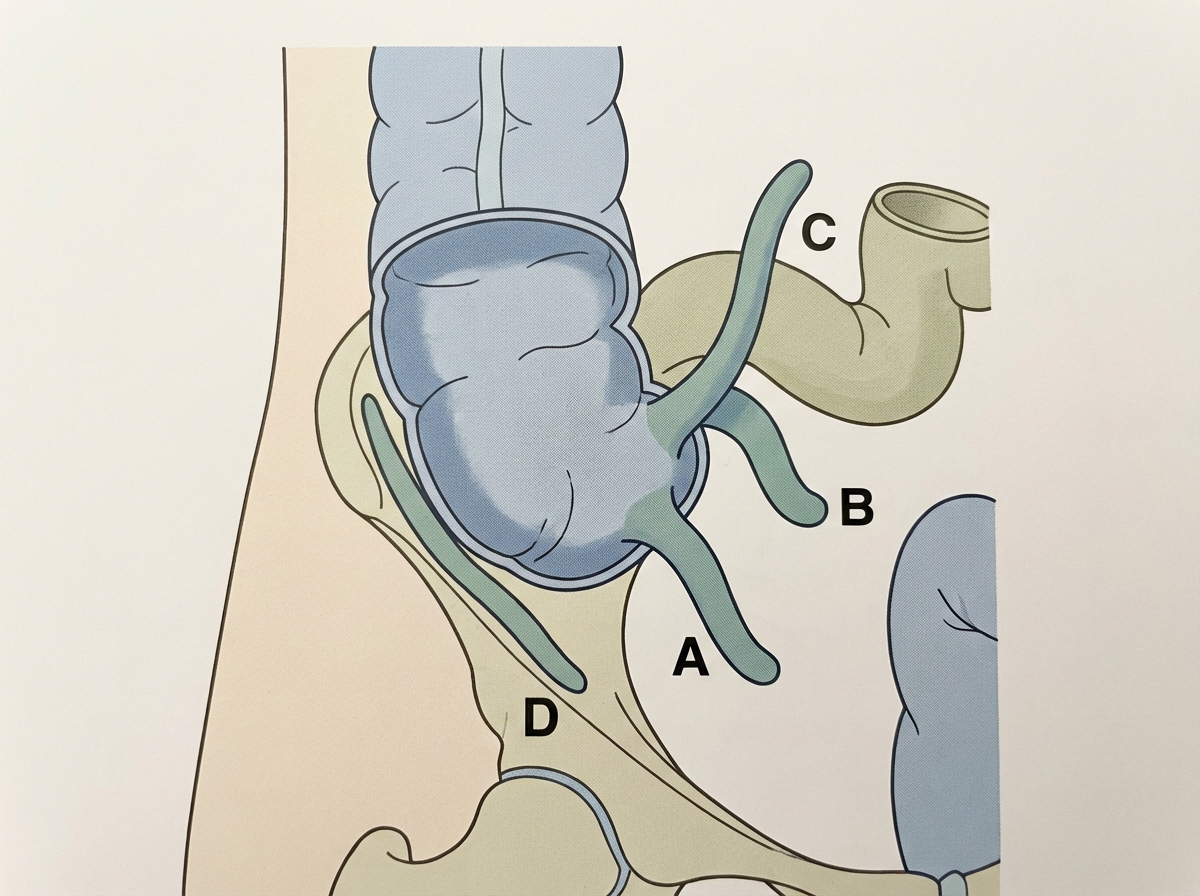
A 20-year-old male patient presented to the ER with complaints of abdominal pain, nausea, and vomiting. The pain was initially peri-umbilical in nature; however, with time, the pain worsened and shifted to the right lower quadrant. On palpating the abdomen, tenderness is present over the right lower quadrant with guarding. The patient is febrile and lab reports show leukocytosis. An emergency laparotomy is planned, and the inflamed organ is identified by the confluence of taenia coli. Which position of the above-mentioned organ is considered to be the most dangerous position (i.e., greatest risk of delayed clinical recognition)?
Meckel's diverticulitis is indistinguishable at the bedside from which of the following conditions?
Which of the following conditions is NOT associated with a 'jelly belly' appearance?
Patients at increased risk for gastric carcinoma include all of the following EXCEPT?
What is the treatment for a bleeding benign gastric ulcer?
A 70-year-old patient presents with symptoms of achalasia for 3 months. Radiologic features and manometric studies show the typical features of achalasia. What is the next step in management?
A 60-year-old man presents with epigastric pain after meals, with some nausea and vomiting. A burning sensation in the midepigastrium is relieved by antacids and H2 antagonists. Upper endoscopy demonstrates paired ulcers on both walls of the proximal duodenum. Which of the following represents the most common complication of this patient's duodenal disease?
Practice by Chapter
Esophageal Disorders
Practice Questions
Gastric Disorders
Practice Questions
Small Intestine Pathology
Practice Questions
Appendicitis
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Intestinal Obstruction
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Diverticular Disease
Practice Questions
Anorectal Disorders
Practice Questions
Colorectal Neoplasms
Practice Questions
Gastrointestinal Stomas
Practice Questions
Bariatric Surgery Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app