
Gastrointestinal Surgery — MCQs

On this page
In which of the following conditions is Alvarado score indicated?
Howship-Romberg sign is seen in
A 60-year-old man presents with foul breath and regurgitates food eaten 3 days ago. What is the most likely diagnosis?
Hamman's sign is seen in which of the following conditions?
Forrest classification is used for evaluating:
In a female with appendicitis in pregnancy the treatment of choice is:
Most common cause of esophageal perforation at the site of cricopharynx -
Alvarado score is used for
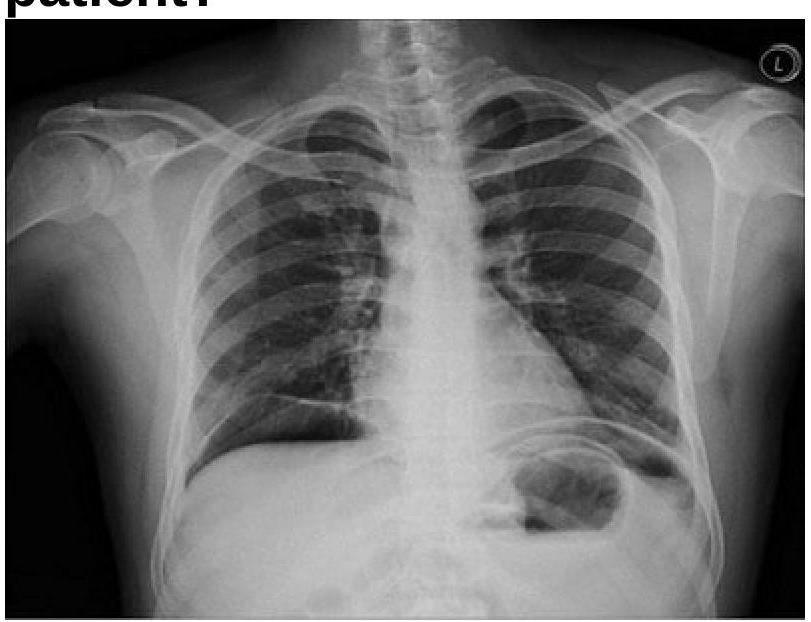
A 40 years old male was brought emergency with severe abdominal pain. On examination, pulse rate was 112/minute and systolic BP was 80 mmHg. Chest x-ray is given below. What is the most appropriate management?
Cushing ulcers are:-
Practice by Chapter
Esophageal Disorders
Practice Questions
Gastric Disorders
Practice Questions
Small Intestine Pathology
Practice Questions
Appendicitis
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Intestinal Obstruction
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Diverticular Disease
Practice Questions
Anorectal Disorders
Practice Questions
Colorectal Neoplasms
Practice Questions
Gastrointestinal Stomas
Practice Questions
Bariatric Surgery Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app