
Gastrointestinal Surgery — MCQs

On this page
Which of the following is the most commonly performed repair for a direct inguinal hernia?
A surgeon examined the case of hernia. Forcefully reduces the sac in abdominal cavity, without actually pushing back the contents. Identify the type of hernia.
A 23-year-old man presents to the emergency department with bloody vomitus. The patient is an alcoholic and has presented similarly before. He is given ondansetron; however, he continues to vomit. The patient complains of sudden substernal chest pain and dysphagia after another bout of vomiting. His temperature is 99°F (37.2°C), blood pressure is 117/60 mmHg, pulse is 122/min, respirations are 15/min, and oxygen saturation is 99% on room air. Physical exam is notable for an uncomfortable man with subcutaneous emphysema in the patient’s neck and supraclavicular areas. Which of the following is the most likely diagnosis?
A 25-year-old man presents to his gastroenterologist for trouble swallowing. The patient states that whenever he eats solids, he regurgitates them back up. Given this patient's suspected diagnosis, the gastroenterologist performs a diagnostic test. Several hours later, the patient presents to the emergency department with chest pain and shortness of breath. His temperature is 99.5°F (37.5°C), blood pressure is 130/85 mmHg, pulse is 60/min, respirations are 12/min, and oxygen saturation is 99% on room air. On physical exam, the patient demonstrates a normal cardiopulmonary exam. His physical exam demonstrates no tenderness of the neck, a normal oropharynx, palpable crepitus above the clavicles, and minor lymphadenopathy. Which of the following is the best next step in management?
Which of the following is not done in carcinoma esophagus?
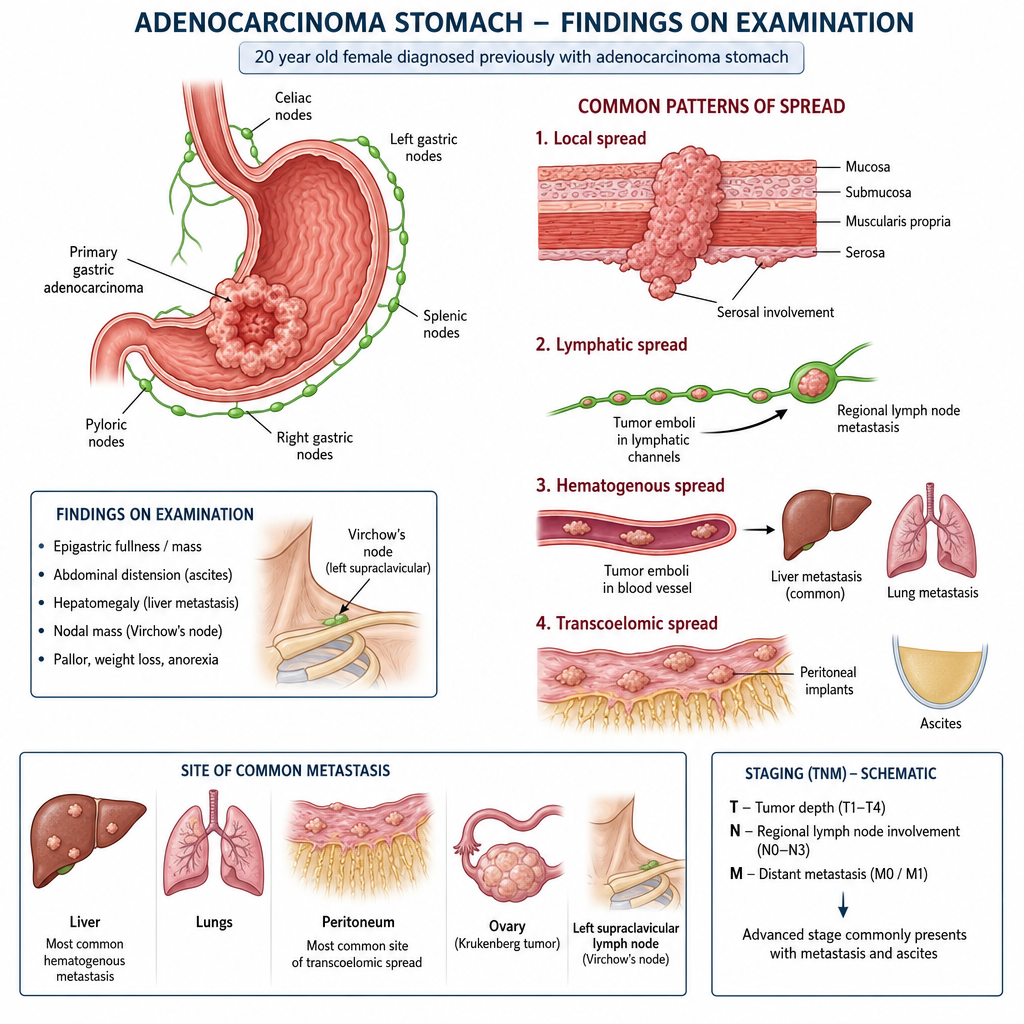
20 yr old female diagnosed previously with adenocarcinoma stomach and on examination following is seen;
Surgery is indicated in Ulcerative Colitis in all except?
In gastric outlet obstruction in a peptic ulcer patient, the site of obstruction is most likely to be:
A patient who underwent gastrectomy develops sweating and diarrhea within 20 minutes after eating. What could be the cause?
A patient presents with acute appendicitis. What is NOT to be done?
Practice by Chapter
Esophageal Disorders
Practice Questions
Gastric Disorders
Practice Questions
Small Intestine Pathology
Practice Questions
Appendicitis
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Intestinal Obstruction
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Diverticular Disease
Practice Questions
Anorectal Disorders
Practice Questions
Colorectal Neoplasms
Practice Questions
Gastrointestinal Stomas
Practice Questions
Bariatric Surgery Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app