
Gastrointestinal Surgery — MCQs

On this page
Valentino's syndrome is:
'Swiss cheese defects' are seen during laparoscopic repair of:
All of the following are sequelae of peptic ulcer surgery EXCEPT:
A 22-year female has presented with a history of malaise, cough, alternating constipation and diarrhoea with intermittent abdominal pain for last 6 months. She also complains of abdominal distension for last 2 days. On examination her abdomen has a doughy feel along with an ill defined mass over the right lower quadrant. She is most likely suffering from:
A 38-year-old man with Crohn's disease presents with a 3-day history of increasing abdominal pain, distension, and inability to pass gas or stool. CT shows dilated small bowel loops with a transition point in the terminal ileum and bowel wall thickening. What factor most influences the decision between conservative and surgical management?
A 28-year-old woman presents with right lower quadrant pain, nausea, and fever. CT shows appendiceal wall thickening and fat stranding. Her white blood cell count is 13,000/μL with 85% neutrophils. However, she is 12 weeks pregnant. What is the most appropriate management considering the clinical scenario?
A 28-year-old pregnant woman at 32 weeks gestation presents with acute appendicitis. She is hemodynamically stable but has significant right lower quadrant pain and leukocytosis. The obstetric team is concerned about preterm labor risk, while the surgical team recommends immediate appendectomy. Synthesize the risks and benefits to determine the optimal management approach.
A patient presents with an umbilical mass, which was previously reducible but has now become irreducible with serosanguinous (non-purulent, non-enteric) discharge coming out, as shown in the image. On examination, the overlying skin shows ischemic changes but no signs of active infection, cellulitis, or abscess. Urgent exploration confirms viable bowel, a small (2 cm) fascial defect, no enteric spillage, and no gross contamination; the wound is classified as clean-contaminated. There are no signs of perforated or strangulated bowel. What is the most appropriate management?

Which of the following is not seen with ileal resections?
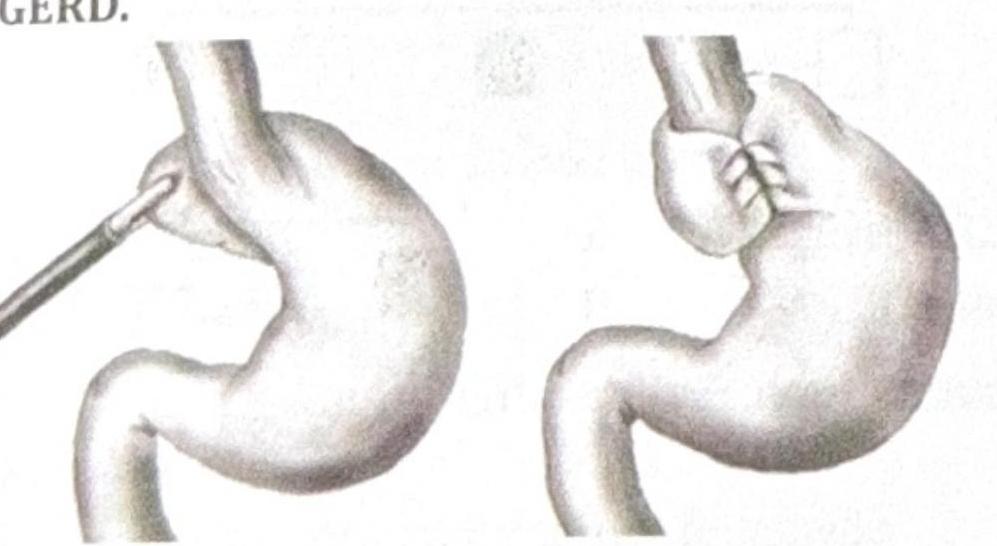
Identify the procedure shown in the image, which is performed in a patient with recurrent GERD.
Practice by Chapter
Esophageal Disorders
Practice Questions
Gastric Disorders
Practice Questions
Small Intestine Pathology
Practice Questions
Appendicitis
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Intestinal Obstruction
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Diverticular Disease
Practice Questions
Anorectal Disorders
Practice Questions
Colorectal Neoplasms
Practice Questions
Gastrointestinal Stomas
Practice Questions
Bariatric Surgery Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app