
Gastrointestinal Surgery — MCQs

On this page
Gastric conduit after oesophageal resection is based upon:
A 45 year old female patient presents with a painless firm abdominal swelling of size 10 x 8 cm near the umbilicus. The swelling is reducible and shows no fixation to deeper structures. The most probable clinical diagnosis in this patient is
A 35 year old male patient with enteric fever presents to the emergency with sudden onset of generalised abdominal pain, abdominal distension, nausea, vomiting and constipation for last 48 hours. On examination, patient is dehydrated with PR = 110/min and BP = 100/60 mm Hg. There is generalised tenderness, rebound tenderness present and board like rigidity on per abdomen examination. The most likely complication of enteric fever in this patient is
Which of the following statements with regard to Enteric perforation are correct? 1. Salmonella typhi is the causative organism for Enteric fever 2. Enteric perforation characteristically occurs during the third week of illness 3. Typhoid ulcers are placed transversely to the long axis of the gut 4. Terminal ileum is the most common site for enteric perforation
Which of the following is NOT a classical symptom of acute appendicitis ?
Which one of the following is given a score of two in Alvarado score?
An air fluid level with dilated oesophagus and “bird beak” appearance in a barium swallow is diagnostic of:
Which one of the following statements is not correct regarding trichobezoar ( hair balls)?
What is the treatment of choice in a patient with Crohn’s disease, where inflamed appendix was found on exploration?
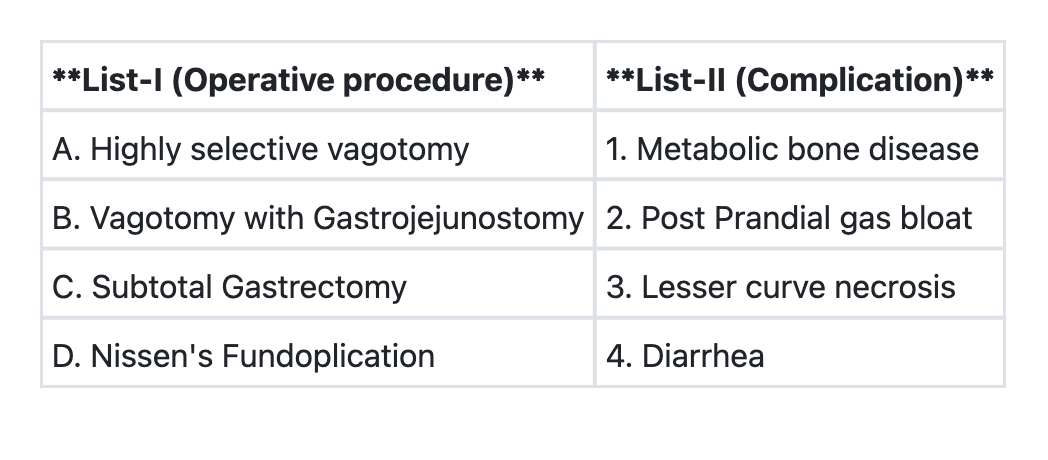
Match List-I with List-II and select the correct answer using the code given below the Lists: **List-I (Procedure)** A. Highly selective vagotomy B. Vagotomy with gastrojejunostomy C. Subtotal gastrectomy D. Nissen's fundoplication **List-II (Complication)** 1. Metabolic bone disease 2. Post-prandial gas bloat 3. Lesser curve necrosis 4. Diarrhea **Code:**
Practice by Chapter
Esophageal Disorders
Practice Questions
Gastric Disorders
Practice Questions
Small Intestine Pathology
Practice Questions
Appendicitis
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Intestinal Obstruction
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Diverticular Disease
Practice Questions
Anorectal Disorders
Practice Questions
Colorectal Neoplasms
Practice Questions
Gastrointestinal Stomas
Practice Questions
Bariatric Surgery Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app