
Gastrointestinal Surgery — MCQs

On this page
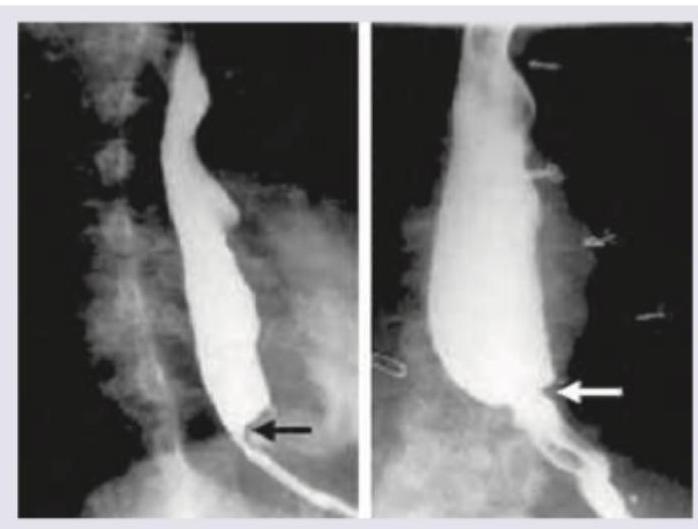
All the following statements regarding this film representing esophagus are true except:
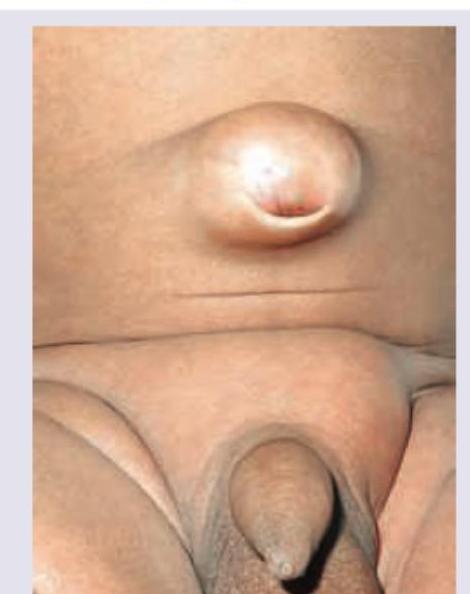
A 35-year-old patient presents with a painless swelling at the umbilicus that has been gradually increasing in size over the past 6 months. The swelling increases on coughing and straining. On examination, there is a reducible bulge at the umbilicus, and the fascial defect is noted to pass directly through the umbilical ring. What is the likely diagnosis?
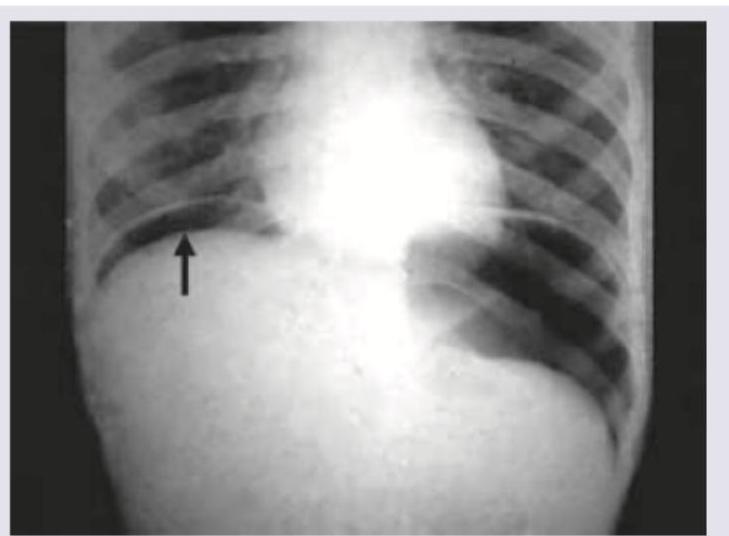
A 30-year-old patient presents with abdominal pain, fever, nausea, vomiting and respiratory distress. On admission BP=80/40 mm Hg and pulse rate is 120 BPM. The following CXR was performed. What is the immediate management? (AIIMS May 2016)
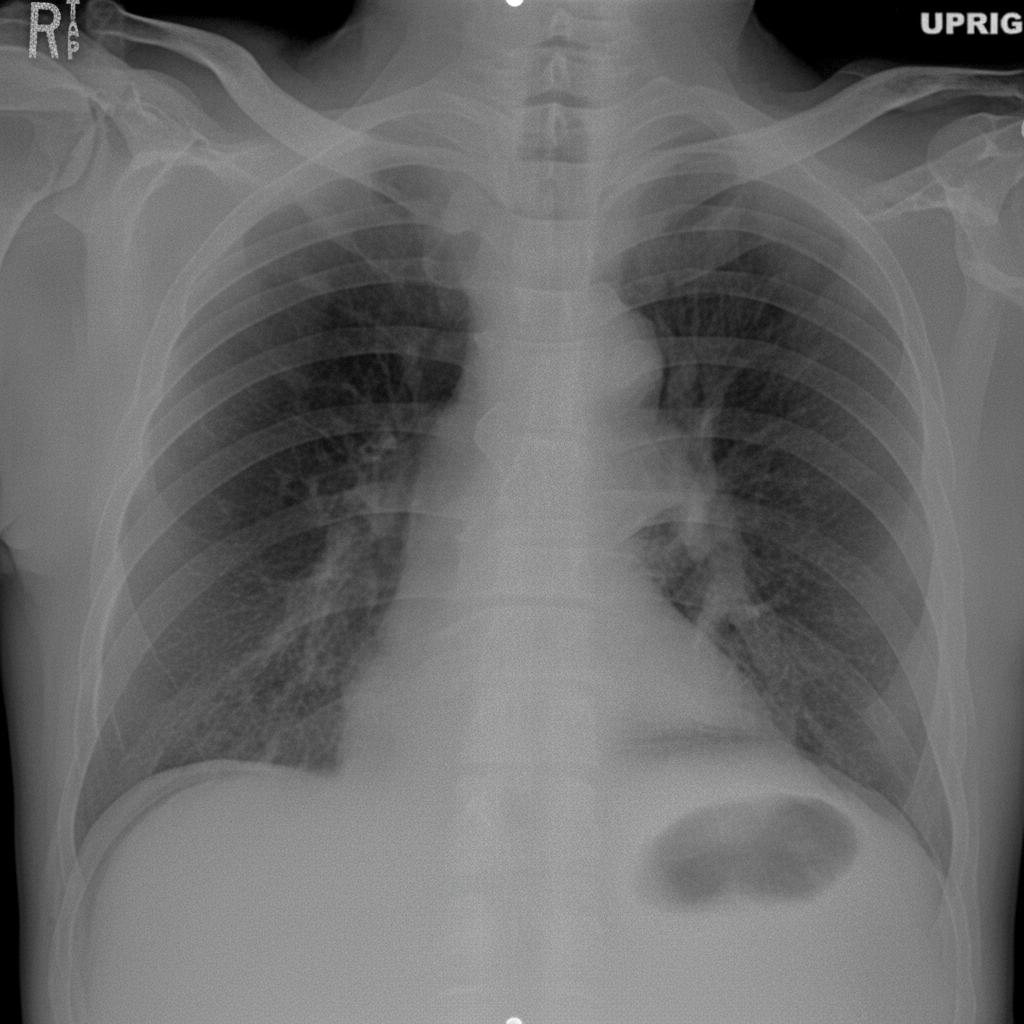
Which is correct about hematemesis (upper GI bleeding) in this patient?

Based on the X-ray findings, what is the underlying diagnosis?
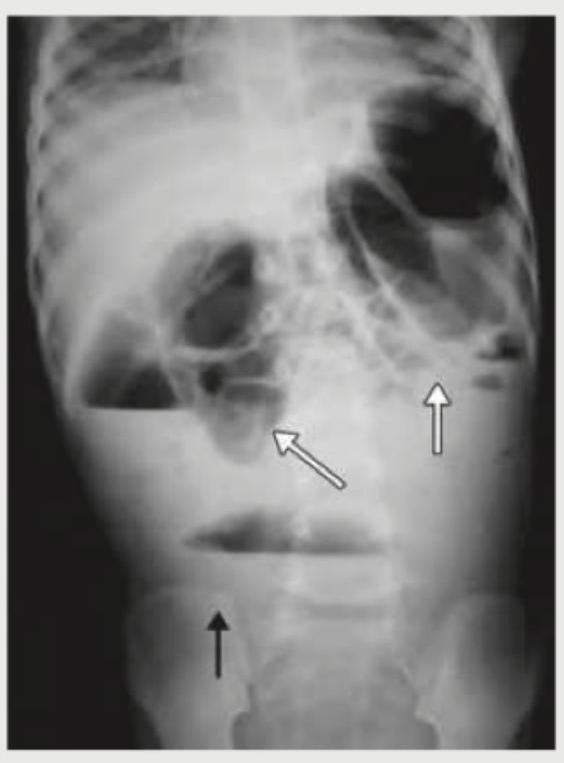
The following X-ray abdomen is diagnostic of:
All of the following statements regarding this radiological film representing esophagus are true except:

Which one of the following statements is not correct regarding Gastric outlet obstruction associated with long standing peptic ulcer disease?
Which of the following are correct regarding late dumping? I. It usually occurs during the second hour after meal. II. It lasts for 30-40 minutes. III. Major symptoms are tremor, faintness, prostration IV. It is relieved by lying down. Select the answer using the code given below :
While managing oesophageal perforations, which of the following factors favour non-operative management? 1. Perforation by a flexible endoscope 2. Contained perforation without free communication 3. Perforation with a small septic load 4. Perforation of the abdominal oesophagus Select the correct answer using the code given below:
Practice by Chapter
Esophageal Disorders
Practice Questions
Gastric Disorders
Practice Questions
Small Intestine Pathology
Practice Questions
Appendicitis
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Intestinal Obstruction
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Diverticular Disease
Practice Questions
Anorectal Disorders
Practice Questions
Colorectal Neoplasms
Practice Questions
Gastrointestinal Stomas
Practice Questions
Bariatric Surgery Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app