
Gastrointestinal Surgery — MCQs

On this page
Which of the following procedures has the highest risk of causing the recurrence of duodenal ulcers?
A 60-year-old male with a history of peptic ulcer disease presents with sudden-onset severe epigastric pain radiating to the back, vomiting, and shock. Examination reveals a rigid, board-like abdomen. Upright chest X-ray shows air under both hemidiaphragms. What is the most appropriate initial surgical management?
A 25-year-old male presents with pain starting from the umbilicus moving to the right iliac fossa, associated with fever, nausea, and tenderness in the right iliac fossa. His WBC count is 14,000/cmm. What is the Alvarado score?
Which of the following is wrongly matched with its classification?
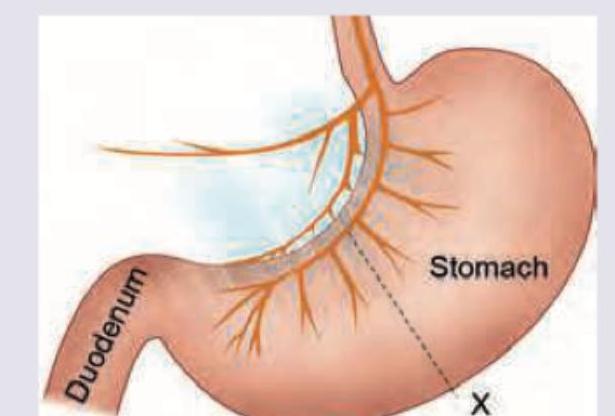
Which nerve marked as $X$ is shown in the image given below? (Recent NEET Pattern 2016-17)
All of the following conditions are visible in the image except: (Recent NEET Pattern 2016-17)
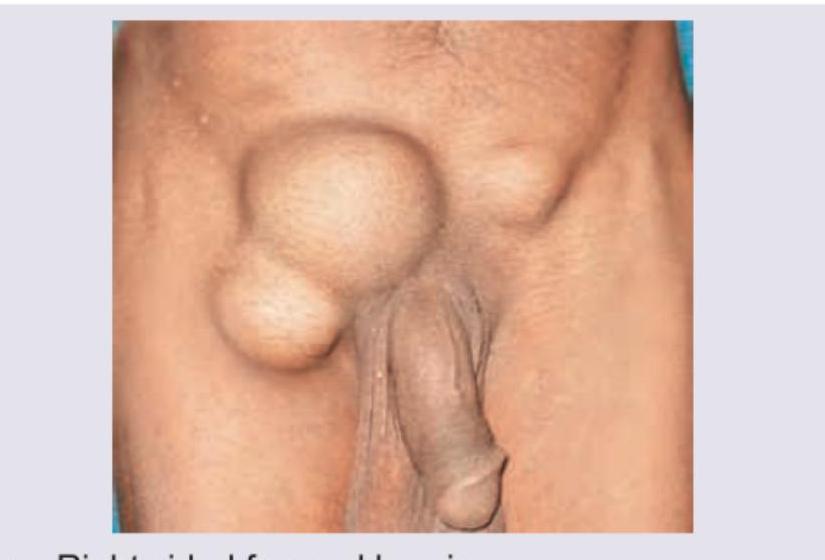
A multiparous female presents with the condition shown in the image. This condition can be managed by: (Recent NEET Pattern 2016-17)

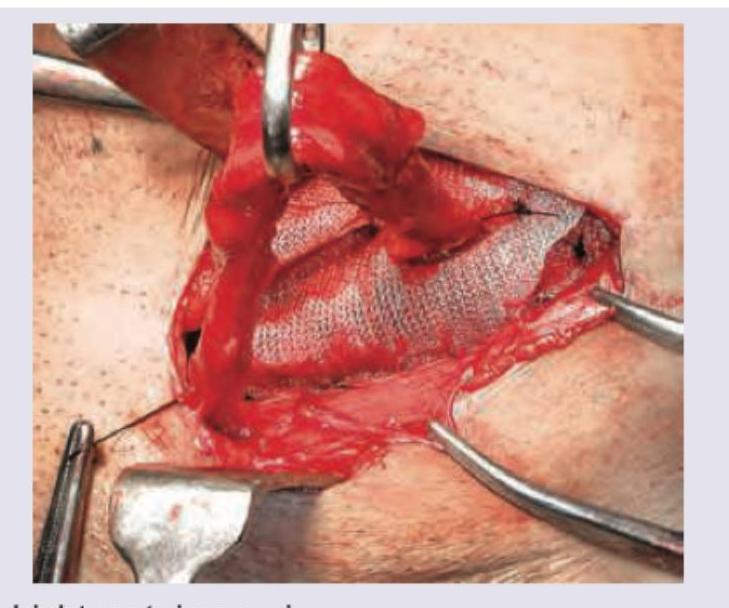
Which hernia repair procedure is shown in the image? (Recent NEET Pattern 2016-17)
A 25-year-old male presents with inguinal swelling. He had surgery for acute abdomen 2 years ago but could not tell the reason behind it. Trauma to which structure during the surgery conducted 2 years ago would have resulted in this inguinal swelling?
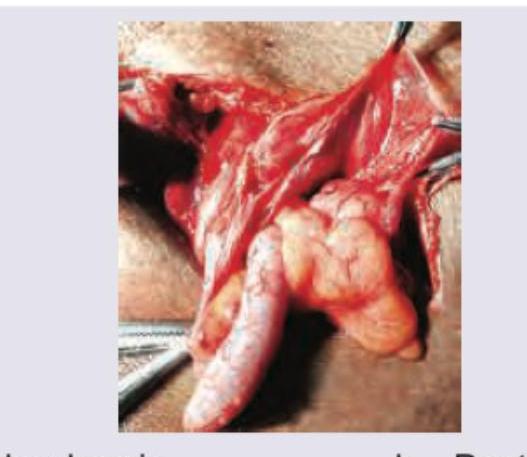
Contents of the inguinal hernia sac are displayed intraoperatively and appendix is seen at 7 o'clock. What is the diagnosis?
Practice by Chapter
Esophageal Disorders
Practice Questions
Gastric Disorders
Practice Questions
Small Intestine Pathology
Practice Questions
Appendicitis
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Intestinal Obstruction
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Diverticular Disease
Practice Questions
Anorectal Disorders
Practice Questions
Colorectal Neoplasms
Practice Questions
Gastrointestinal Stomas
Practice Questions
Bariatric Surgery Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app