
Gastrointestinal Surgery — MCQs

On this page
All are true statements about Meckel's diverticulum except?
What is true of pepsinogen?
Extensive ileal resection can cause all of the following EXCEPT:
Which condition is characterized by the presence of odorless peritoneal fluid?
Paralytic ileus is caused by which of the following conditions?
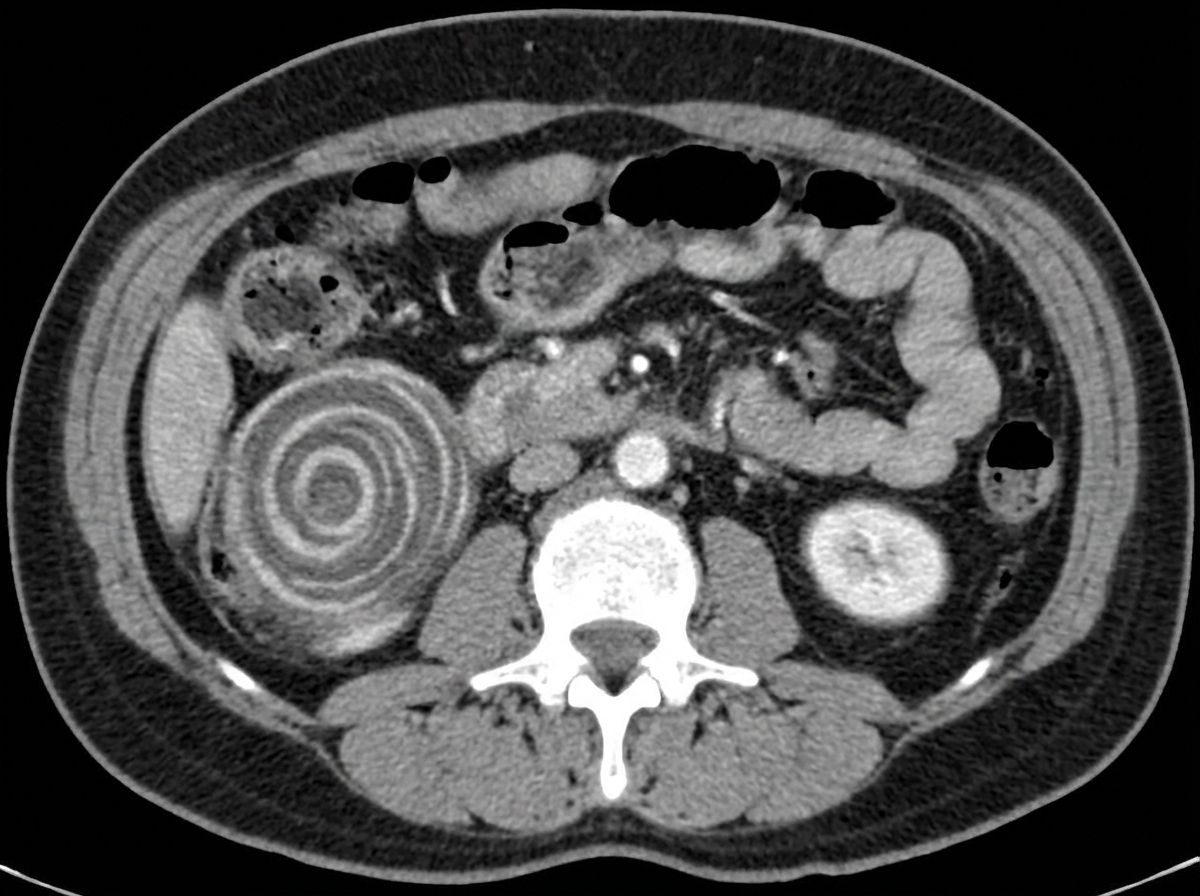
A 45-year-old adult male presents with colicky abdominal pain, nausea, and vomiting for 3 days. CT abdomen reveals the characteristic "target sign" consistent with colonic intussusception with a discrete lead point and dilated proximal bowel loops. He is hemodynamically stable with viable bowel and no evidence of perforation or gross contamination. What is the treatment of choice for this patient?
What is typically NOT seen following a massive resection of the small bowel?
Hourglass stomach is seen in which of the following conditions?
Post-vagotomy diarrhea can be effectively managed by which of the following?
Which of the following is NOT a complication of chronic duodenal ulcer?
Practice by Chapter
Esophageal Disorders
Practice Questions
Gastric Disorders
Practice Questions
Small Intestine Pathology
Practice Questions
Appendicitis
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Intestinal Obstruction
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Diverticular Disease
Practice Questions
Anorectal Disorders
Practice Questions
Colorectal Neoplasms
Practice Questions
Gastrointestinal Stomas
Practice Questions
Bariatric Surgery Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app