
Gastrointestinal Surgery — MCQs

On this page
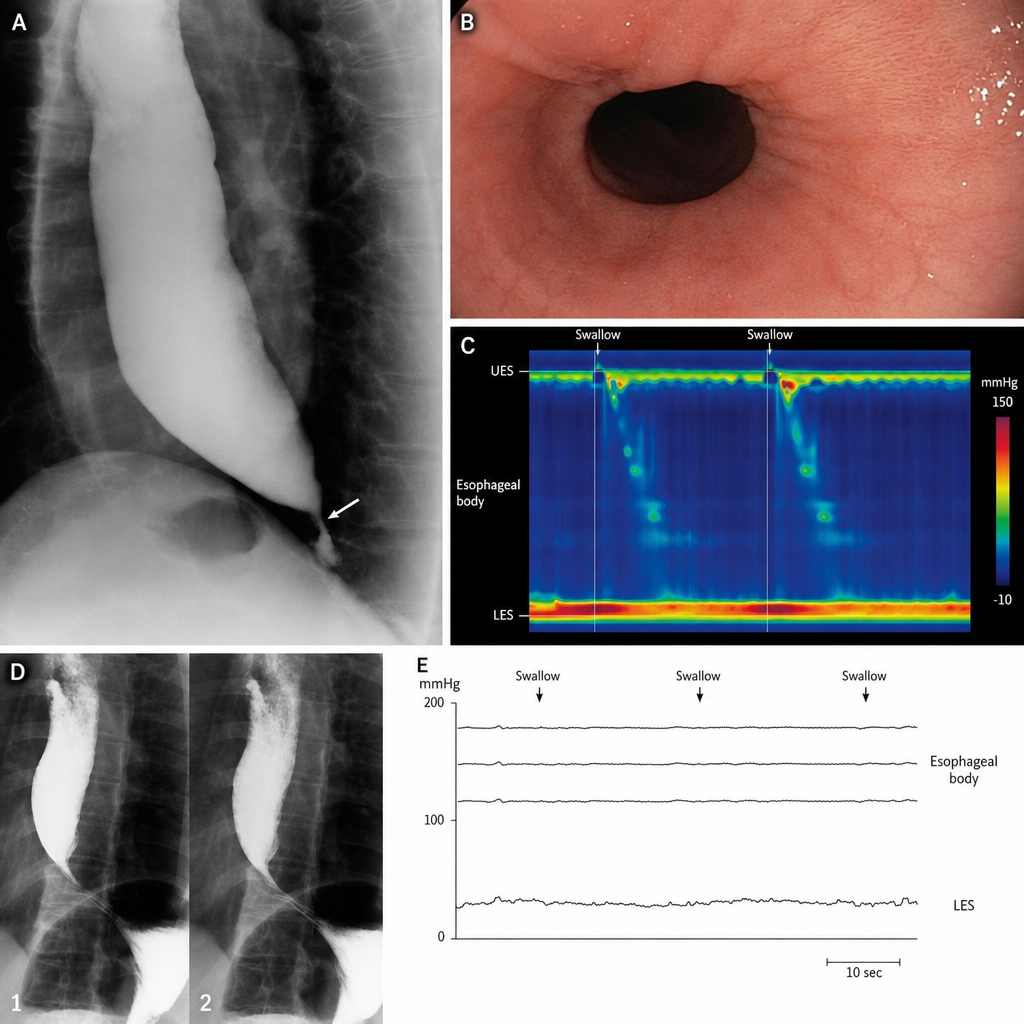
Regarding Achalasia Cardia, which of the following statements are true? 1. The hallmark pathophysiology is the loss of inhibitory postganglionic neurons (which release Nitric Oxide and VIP) in the myenteric plexus, leading to impaired LES relaxation and absent normal peristalsis. 2. Dysphagia characteristically occurs for both solids and liquids from the onset. 3. Barium swallow typically shows a "Corkscrew esophagus" appearance due to persistent narrowing at the GE junction with proximal dilatation. 4. Manometry is the Gold Standard for diagnosis, with key findings of incomplete LES relaxation (elevated Integrated Relaxation Pressure above the system-specific threshold on high-resolution manometry) and aperistalsis in the smooth muscle portion of the esophagus. 5. The most common cancer associated with Achalasia is Adenocarcinoma.
All of the following are indications for surgery in a case of duodenal ulcer except?
Which of the following statements about carcinoid of the appendix is NOT TRUE?
Malignant transformation is commonly seen in which type of ulcer?
All are true about acute appendicitis except:
Highest incidence of acute appendicitis occurs in which decade of life?
As per EHS classification, what is the designation for a primary, direct inguinal hernia with a 4 cm width?
All of the following are early complications arising after appendicectomy for acute appendicitis except?
What is the treatment of choice for a bleeding gastric ulcer?
A 64-year-old male presented with severe diarrhea, having more than 20 bowel movements per day, following an elective operation for duodenal ulcer disease. Medications have been ineffective. The exact details of his operation cannot be ascertained. What operation was most likely performed?
Practice by Chapter
Esophageal Disorders
Practice Questions
Gastric Disorders
Practice Questions
Small Intestine Pathology
Practice Questions
Appendicitis
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Intestinal Obstruction
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Diverticular Disease
Practice Questions
Anorectal Disorders
Practice Questions
Colorectal Neoplasms
Practice Questions
Gastrointestinal Stomas
Practice Questions
Bariatric Surgery Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app